

The many faces of facial nerve schwannoma
- PMID: 16552018
- PMCID: PMC7976970
The many faces of facial nerve schwannoma
Abstract
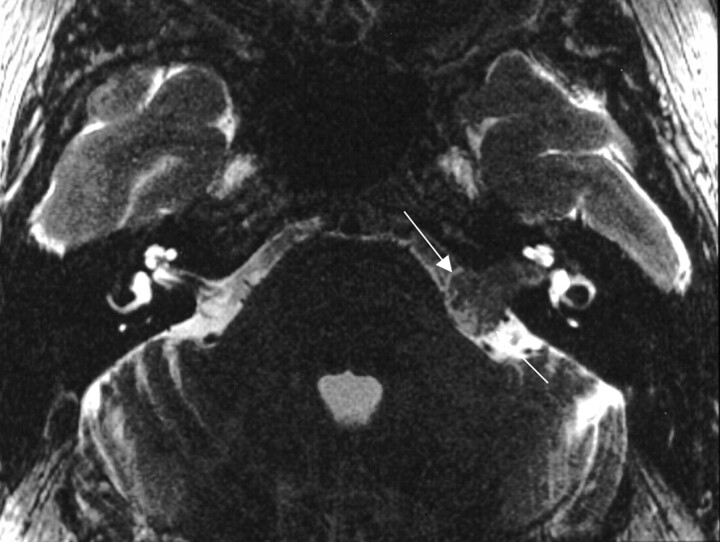
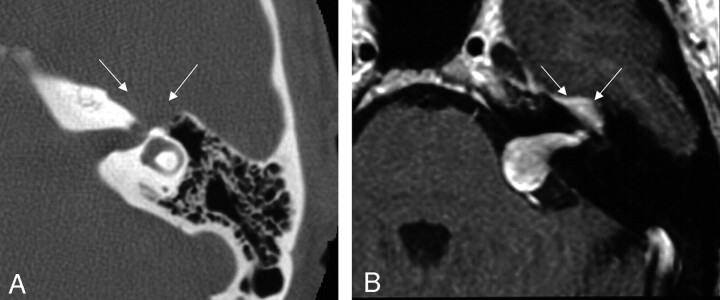
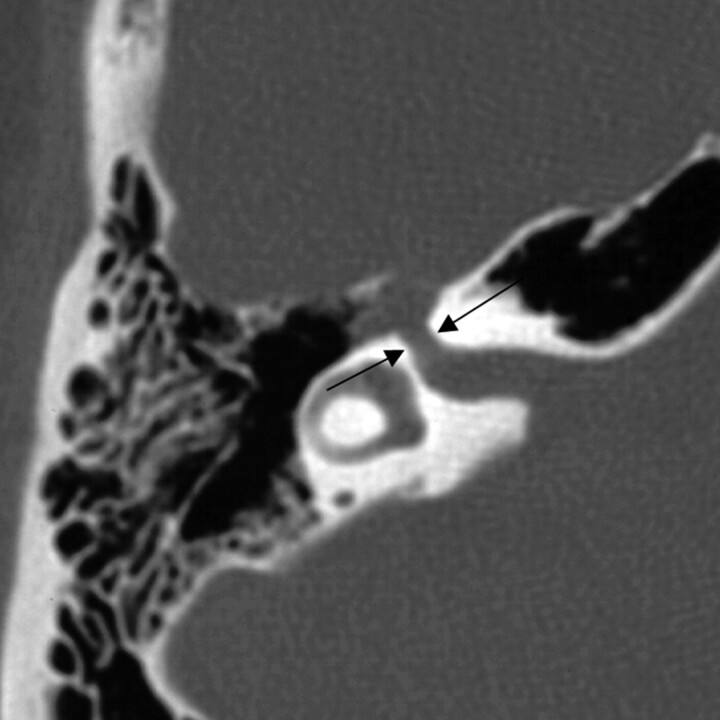
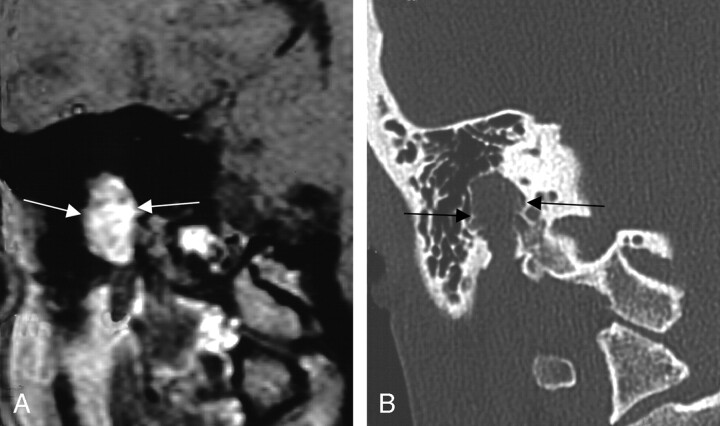
Background and purpose: The imaging appearance of facial nerve schwannomas (FNSs) has been described as an enhancing tubular mass (using T1-enhanced MR) within an enlarged facial nerve canal (using CT). The purpose of this study is to identify how often the FNS imaging findings conform to this description and determine whether there are underlying anatomic explanations for the discrepant imaging appearances identified.
Materials and methods: The clinical, pathologic, and radiologic records of 24 FNS in 23 patients were retrospectively reviewed. Each FNS was evaluated for location along the facial nerve. The lesions were cataloged by facial nerve segment with the imaging characteristics of each segment described.
Results: The average age at time of first imaging was 39 years (age range, 10-70 years). Eighteen (71%) of the 24 FNSs were pathologically confirmed, while the others were determined intraoperatively or diagnostically by the presence of both enlargement of the facial nerve canal and enhancement on contrast-enhanced T1 MR examination. The most common location was in the geniculate fossa (83%), followed by the labyrinthine and tympanic segments of the facial nerve (both 54%). The most common clinical presentation was facial neuropathy (42%).
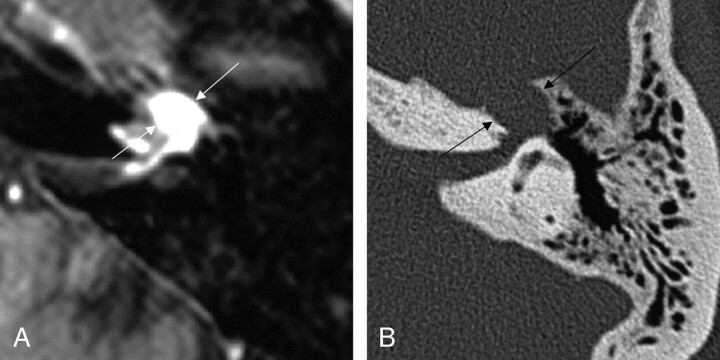
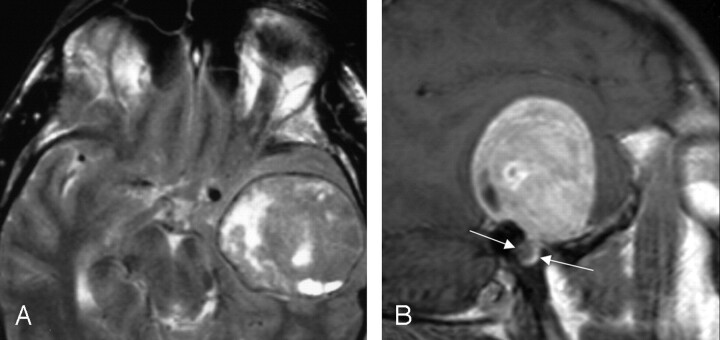
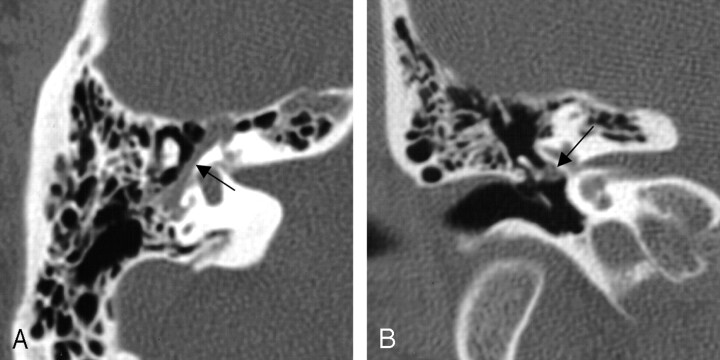
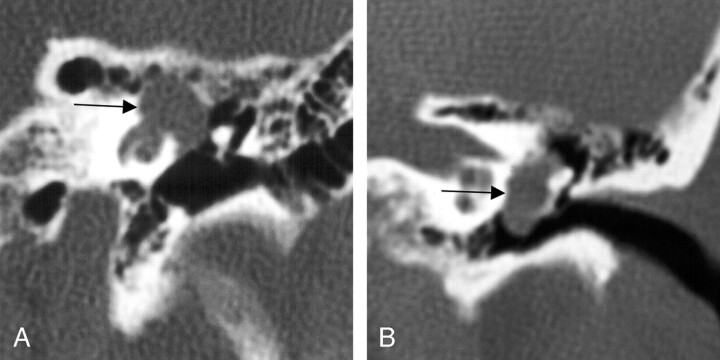
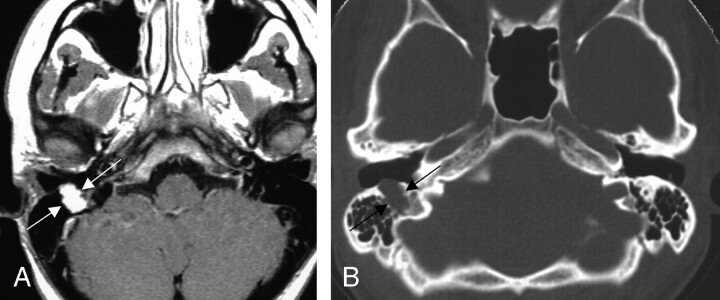
Conclusion: The classic description of FNS on enhanced T1 MR is that of a well-circumscribed fusiform enhancing mass along the course of the intratemporal facial nerve with bone algorithm CT showing sharply defined bony canal enlargement. Modern imaging techniques, however, demonstrate the importance of the surrounding anatomic landscape, leading to various imaging appearances. Lesions traversing the labyrinthine segment can demonstrate a dumbbell appearance. When FNSs track along the greater superficial petrosal nerve, they may present as a round mass projecting up into the middle cranial fossa. FNS of the tympanic segment of the facial nerve preferentially pedunculate into the middle ear cavity, clinically presenting as a middle ear mass. When the mastoid segment of the facial nerve is involved, irregular and "invasive" tumor margins seen on MR can be explained on CT as tumor breaking into surrounding mastoid air cells.
Figures
Comment in
-
Dural tail: another face of facial nerve schwannoma?AJNR Am J Neuroradiol. 2006 Oct;27(9):1804; author reply 1805. AJNR Am J Neuroradiol. 2006. PMID: 17032843 Free PMC article. No abstract available.
References
-
- O’Donoghue GM, Brackmann DE, House JW, et al. Neuromas of the facial nerve. Am J Otol 1989;10:49–54 - PubMed
-
- Symon L, Cheesman AD, Kawauchi M, et al. Neuromas of the facial nerve: a report of 12 cases. Br J Neurosurg 1993;7:13–22 - PubMed
-
- Chung SY, Kim DI, Lee BH, et al. Facial nerve schwannomas: CT and MR findings. Yonsei Med J 1998;39:148–53 - PubMed
-
- Balle VH, Greisen O. Neurilemmomas of the facial nerve presenting as parotid tumors. Ann Otol Rhinol Laryngol 1984;93:70–72 - PubMed
-
- Lidov M, Som PM, Stacy C, et al. Eccentric cystic facial schwannoma: CT and MR features. J Comp Axial Tomgr 1991;15:1065–67 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical