

Laparoscopic liver resection for peripheral hepatocellular carcinoma in patients with chronic liver disease: midterm results and perspectives
- PMID: 16552201
- PMCID: PMC1448957
- DOI: 10.1097/01.sla.0000206017.29651.99
Laparoscopic liver resection for peripheral hepatocellular carcinoma in patients with chronic liver disease: midterm results and perspectives
Abstract
Objective: Report the midterm results of laparoscopic resection for hepatocellular in chronic liver disease (CLD).
Summary background data: Surgical resection for hepatocellular carcinoma (HCC) in chronic liver disease (CLD) remains controversial because of high morbidity and recurrence rates. Laparoscopic resection of liver tumors has recently been developed and could reduce morbidity.
Methods: From 1998 to 2003, patients with HCC and CLD were considered for laparoscopic liver resection. Inclusion criteria were chronic hepatitis or Child's A cirrhosis, solitary tumor < or =5 cm in size, and location in peripheral segments of the liver. Mortality, morbidity, recurrence rates, and survival were analyzed.
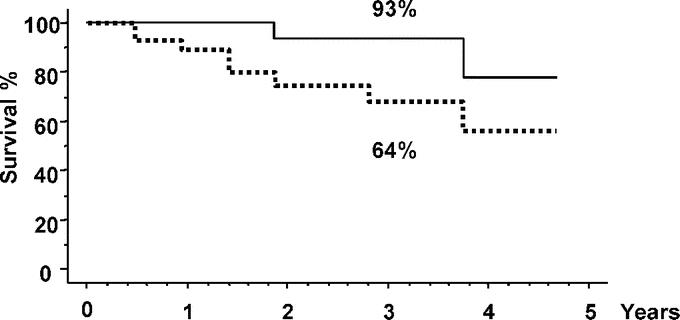
Results: A total of 27 patients were included. Liver resections included anatomic resection in 17 cases and non anatomic resection in 10. Seven conversions to laparotomy (26%) occurred for moderate hemorrhage in 5 cases and technical difficulties in 2 cases. Mortality and morbidity rates were 0% and 33%, respectively. Postoperative ascites and encephalopathy occurred in 2 patients (7%) who both had undergone conversion to laparotomy. Mean surgical margin was 11 mm (range, 1-47 mm). After a mean follow-up of 2 years (range, 1.1-4.7), 8 patients (30%) developed intrahepatic tumor recurrence of which one died. Treatment of recurrence was possible in 4 patients (50%), including orthotopic liver transplantation, right hepatectomy, radiofrequency ablation, and chemoembolization in 1 case each. There were no adhesions in the 2 reoperated patients. Overall and disease-free 3-year survival rates were 93% and 64%, respectively.
Conclusion: Our study shows that laparoscopic liver resection for HCC in selected patients is a safe procedure with very good midterm results. This approach could have an impact on the therapeutic strategy of HCC complicating CLD as a treatment with curative intent or as a bridge to liver transplantation.
Figures
References
-
- Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet. 2003;362:1907–1917. - PubMed
-
- Taylor-Robinson SD, Foster GR, Arora S, et al. Increase in primary liver cancer in the UK, 1979–94. Lancet. 1997;350:1142–1143. - PubMed
-
- Deuffic S, Poynard T, Buffat L, et al. Trends in primary liver cancer. Lancet. 1998;351:214–215. - PubMed
-
- El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med. 1999;340:745–750. - PubMed
-
- Bruix J, Llovet JM. Prognostic prediction and treatment strategy in hepatocellular carcinoma. Hepatology. 2002;35:519–524. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
