

Clinical and economic outcomes of hospital acquired pneumonia in intra-abdominal surgery patients
- PMID: 16552208
- PMCID: PMC1448956
- DOI: 10.1097/01.sla.0000207097.38963.3b
Clinical and economic outcomes of hospital acquired pneumonia in intra-abdominal surgery patients
Abstract
Objective: To measure the clinical and economic impact of postoperative hospital-acquired pneumonia (HAP) and to identify risk factors for the development of HAP.
Summary background data: Although postoperative HAP is recognized to be an major risk associated with surgery, little is known about the overall outcomes of patients whose hospital stay is complicated by HAP following surgery.
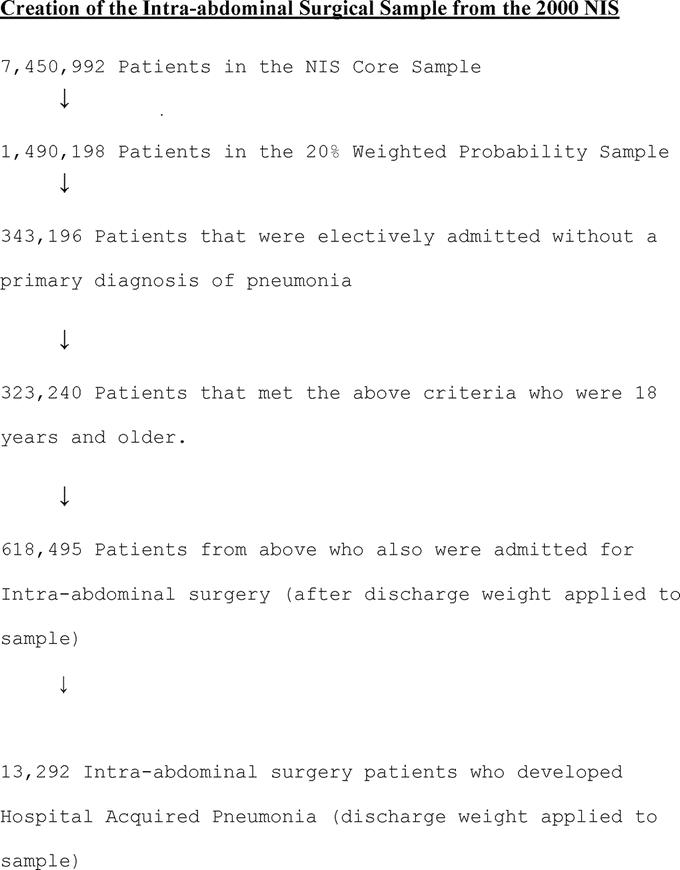
Methods: We studied 618,495 patients who underwent an intra-abdominal operation from the National Inpatient Sample database over a 1-year period (January 2000 to December 2000) using CPT codes and discharge diagnoses identified by the Clinical Classification Software. Data collected included demographic characteristics, type of operation, in-hospital mortality, discharge disposition, length of stay, and hospital charges.
Results: Of the 13,292 patients with HAP following intra-abdominal surgery, 1421 died prior to discharge (mortality = 10.7%) compared with 7217 deaths in the control group of patients without HAP following intra-abdominal surgery (mortality = 1.2%) (P < 0.001). HAP was independently associated with a 4.13-fold (95% confidence interval = 3.94-4.34) increase in risk to be discharged to a skilled nursing facility. The mean length of hospital stay for intra-abdominal patients who developed HAP was significantly greater compared with intra-abdominal surgery patients who did not develop HAP (17.10 days versus 6.07 days, P < 0.001). After adjusting for patient characteristics, HAP was independently associated with a 75% (28,160.95 dollars; 95% confidence interval, 27,543.76 dollars - 28,778.13 dollars) mean increase in total hospital charges.
Conclusions: Given the high incidence and significant impact of HAP on patient outcomes, early preventive strategies and interventions to reduce HAP should be a priority.
Figures
Similar articles
-
Epidemiology and impact of aspiration pneumonia in patients undergoing surgery in Maryland, 1999-2000.Crit Care Med. 2003 Jul;31(7):1930-7. doi: 10.1097/01.CCM.0000069738.73602.5F. Crit Care Med. 2003. PMID: 12847385
-
The burden of Clostridium difficile in surgical patients in the United States.Surg Infect (Larchmt). 2007 Dec;8(6):557-66. doi: 10.1089/sur.2006.062. Surg Infect (Larchmt). 2007. PMID: 18171114
-
In-hospital mortality and morbidity after surgical treatment of unruptured intracranial aneurysms in the United States, 1996-2000: the effect of hospital and surgeon volume.Neurosurgery. 2003 May;52(5):995-1007; discussion 1007-9. Neurosurgery. 2003. PMID: 12699540
-
Oral Health and Hospital-Acquired Pneumonia in Elderly Patients: A Review of the Literature.J Dent Hyg. 2016 Jun;90 Suppl 1:15-21. J Dent Hyg. 2016. PMID: 27458314 Review.
-
Predicting postoperative pulmonary complications: implications for outcomes and costs.Curr Opin Anaesthesiol. 2014 Apr;27(2):201-9. doi: 10.1097/ACO.0000000000000045. Curr Opin Anaesthesiol. 2014. PMID: 24419159 Review.
Cited by
-
Incidence and risk factors of postoperative pulmonary complications in noncardiac Chinese patients: a multicenter observational study in university hospitals.Biomed Res Int. 2015;2015:265165. doi: 10.1155/2015/265165. Epub 2015 Mar 2. Biomed Res Int. 2015. PMID: 25821791 Free PMC article.
-
Decreased Long-Term Respiratory Infection Risk After Bariatric Surgery: a Comprehensive National Cohort Study.Obes Surg. 2021 Feb;31(2):499-507. doi: 10.1007/s11695-020-05001-5. Epub 2020 Sep 28. Obes Surg. 2021. PMID: 32989625
-
Vitamin D's potential to reduce the risk of hospital-acquired infections.Dermatoendocrinol. 2012 Apr 1;4(2):167-75. doi: 10.4161/derm.20789. Dermatoendocrinol. 2012. PMID: 22928073 Free PMC article.
-
Postoperative complications and open gastrectomy affect non-cancer-related death and shorten life expectancy in elderly patients with gastric cancer.Am J Cancer Res. 2021 Oct 15;11(10):5038-5044. eCollection 2021. Am J Cancer Res. 2021. PMID: 34765310 Free PMC article.
-
Multicenter Evaluation of the BioFire FilmArray Pneumonia/Pneumonia Plus Panel for Detection and Quantification of Agents of Lower Respiratory Tract Infection.J Clin Microbiol. 2020 Jun 24;58(7):e00128-20. doi: 10.1128/JCM.00128-20. Print 2020 Jun 24. J Clin Microbiol. 2020. PMID: 32350043 Free PMC article.
References
-
- Cook DJ, Kollef MH. Risk factors for ICU-acquired pneumonia. JAMA. 1998;279:1605–1606. - PubMed
-
- Baker JJ, Lambert RL, Poulos KM, et al. Managing the cost of care: a predictive study to identify critical care patients at risk for nosocomial pneumonia. J Health Care Finance. 2000;26:73–82. - PubMed
-
- Baughman RP, Tapson V, McIvor A. The diagnosis and treatment challenges in nosocomial pneumonia. Diagn Microbiol Infect Dis. 1999;33:131–139. - PubMed
-
- Ephgrave KS, Kleiman-Wexler R, Pfaller M, et al. Postoperative pneumonia: a prospective study of risk factors and morbidity. Surgery. 1993;114:815–819. - PubMed
-
- Fujita T, Sakurai K. Multivariate analysis of risk factors for postoperative pneumonia. Am J Surg. 1995;169:304–307. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
