

Postural hypocapnic hyperventilation is associated with enhanced peripheral vasoconstriction in postural tachycardia syndrome with normal supine blood flow
- PMID: 16565300
- PMCID: PMC4511478
- DOI: 10.1152/ajpheart.01359.2005
Postural hypocapnic hyperventilation is associated with enhanced peripheral vasoconstriction in postural tachycardia syndrome with normal supine blood flow
Abstract
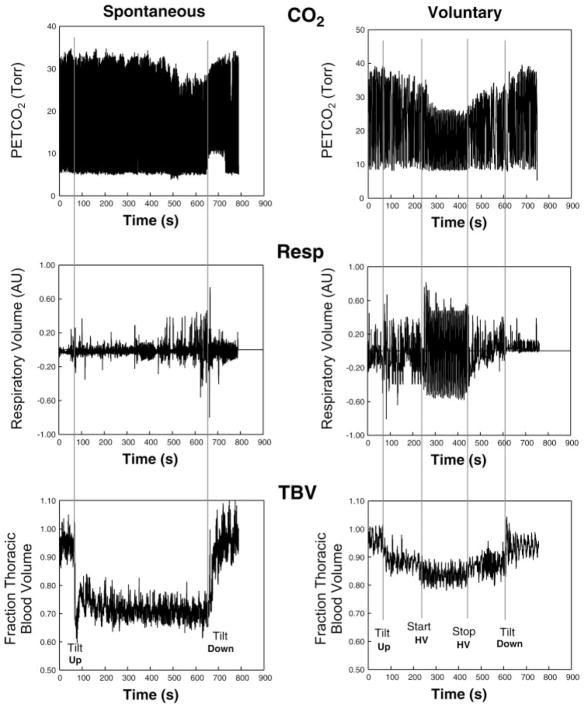
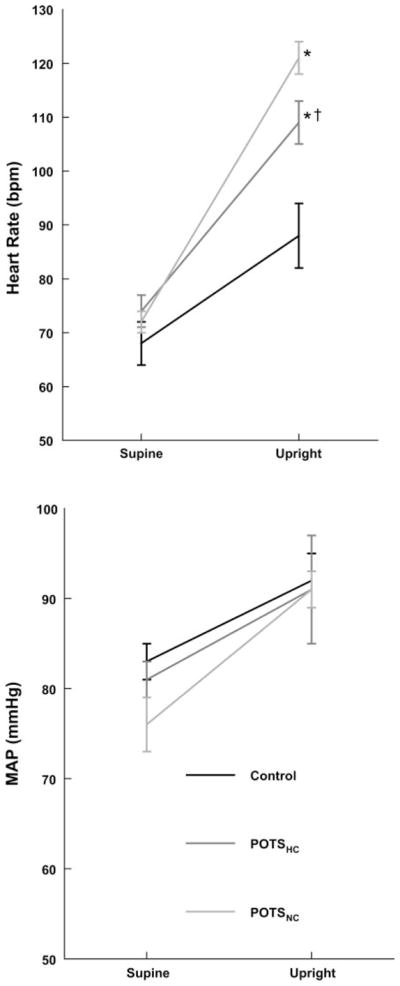
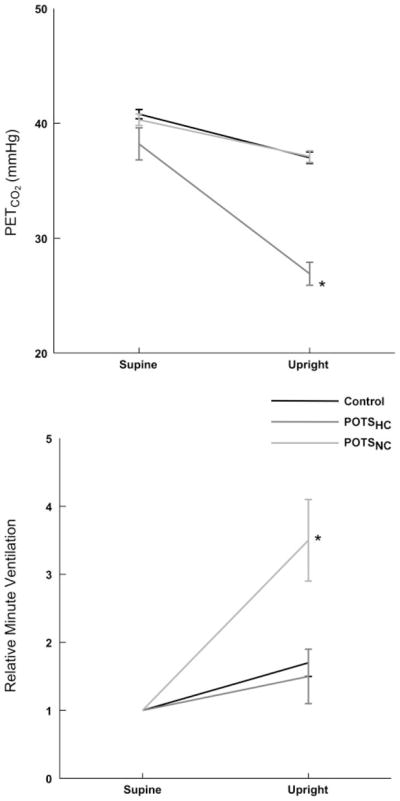
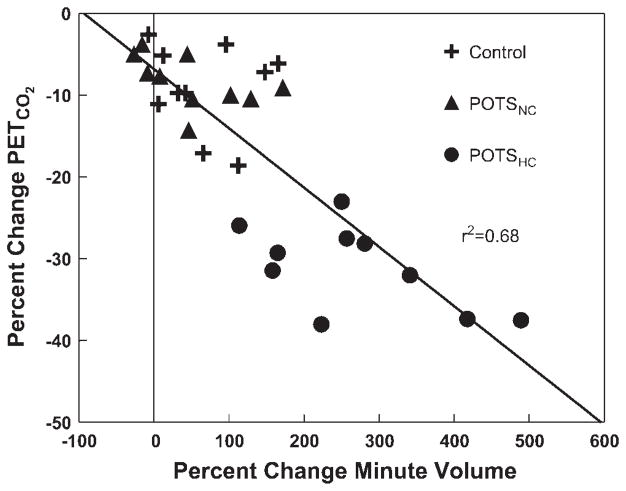
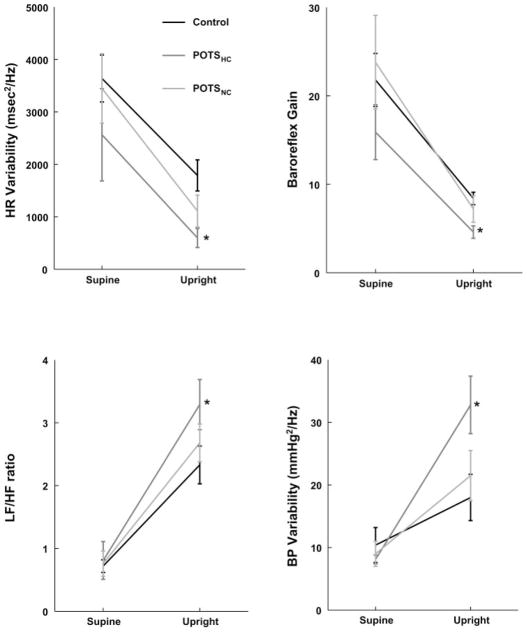
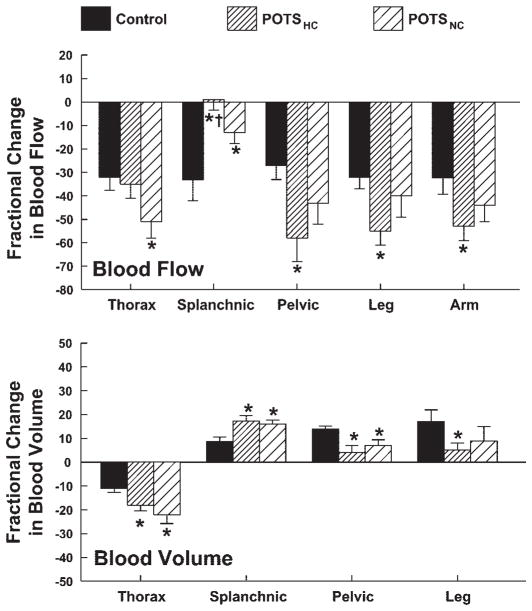
Previous investigations have demonstrated a subset of postural tachycardia syndrome (POTS) patients characterized by normal peripheral resistance and blood volume while supine but thoracic hypovolemia and splanchnic blood pooling while upright secondary to splanchnic hyperemia. Such "normal-flow" POTS patients often demonstrate hypocapnia during orthostatic stress. We studied 20 POTS patients (14-23 yr of age) and compared them with 10 comparably aged healthy volunteers. We measured changes in heart rate, blood pressure, heart rate and blood pressure variability, arm and leg strain-gauge occlusion plethysmography, respiratory impedance plethysmography calibrated against pneumotachography, end-tidal partial pressure of carbon dioxide (Pet(CO2)), and impedance plethysmographic indexes of blood volume and blood flow within the thoracic, splanchnic, pelvic (upper leg), and lower leg regional circulations while supine and during upright tilt to 70 degrees. Ten POTS patients demonstrated significant hyperventilation and hypocapnia (POTS(HC)) while 10 were normocapnic with minimal increase in postural ventilation, comparable to control. While relative splanchnic hypervolemia and hyperemia occurred in both POTS groups compared with controls, marked enhancement in peripheral vasoconstriction occurred only in POTS(HC) and was related to thoracic blood flow. Variability indexes suggested enhanced sympathetic activation in POTS(HC) compared with other subjects. The data suggest enhanced cardiac and peripheral sympathetic excitation in POTS(HC).
Figures
References
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR. Washington, DC: American Psychiatric Association; 2000. (text revision)
-
- Anthonisen NR, Bartlett D, Jr, Tenney SM. Postural effect on ventilatory control. J Appl Physiol. 1965;20:191–196.
-
- Geddes LA, Baker LE. Principles of Applied Biomedical Instrumentation. New York: Wiley; 1989. Detection of physiological events by impedance; pp. 594–600.
-
- Geddes LA, Kidder H. Specific resistance of blood at body temperature II. Med Biol Eng. 1976;14:180–185. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical