

Unequal access to interventional cardiac care in Nova Scotia in patients with acute myocardial infarction complicated by cardiogenic shock
- PMID: 16568158
- PMCID: PMC2560526
- DOI: 10.1016/s0828-282x(06)70918-7
Unequal access to interventional cardiac care in Nova Scotia in patients with acute myocardial infarction complicated by cardiogenic shock
Abstract
Background: The optimal treatment of cardiogenic shock (CS) complicating acute myocardial infarction (AMI) remains controversial and continues to be associated with a high mortality rate. The present study evaluated the outcomes of all patients having AMI complicated by CS in a single Canadian province.
Methods: All consecutive patients diagnosed with AMI and CS from October 1997 to December 2002 in Nova Scotia were included in the present study. The Improving Cardiac Outcomes in Nova Scotia (ICONS) registry was used as the principal source of data. The outcome of interest was in-hospital mortality.
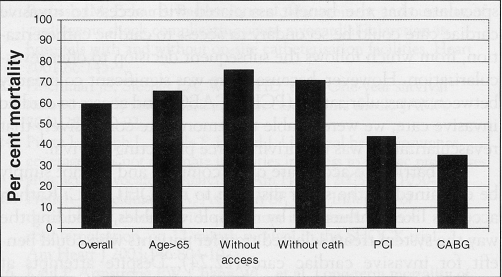
Results: During the study period, a total of 11,300 patients with AMI were identified, with 707 complicated by CS, for an incidence of AMI+CS of 6.3%. The overall mortality rate for patients with AMI+CS was 60.1%. Multivariate regression analysis identified age older than 65 years (OR 2.0; 95% CI 1.4 to 2.9) and renal insufficiency (OR 2.1; 95% CI 1.4 to 3.2) as independent predictors of mortality, while access to invasive cardiac care (defined as admission or transfer to the only cardiac catheterization-capable centre in Halifax, Nova Scotia) was found to be an independent predictor of survival (OR 0.4; 95% CI 0.3 to 0.5). Access to invasive cardiac care was limited to 414 (59%) patients, 250 (35%) of whom actually underwent cardiac catheterization.
Conclusions: Admissions to a tertiary care centre that can provide invasive care was independently associated with improved survival, and older age and renal insufficiency were associated with death among patients with AMI and CS.
HISTORIQUE: Le traitement optimal de l’infarctus aigu du myocarde (IAM) compliqué par un choc cardiogène (CC) demeure controversé et continue de s’associer à un taux de mortalité élevé. La présente étude a évalué l’issue de tous les patients atteints d’un IAM compliqué par un CC dans une seule province du Canada.
MÉTHODOLOGIE: Tous les patients consécutifs atteints d’un IAM et d’un CC diagnostiqués entre octobre 1997 et décembre 2002 en Nouvelle-Écosse ont été inclus dans la présente étude. Le registre du projet ICONS sur l’amélioration des issues cardiovasculaires en Nouvelle-Écosse a servi de source principale de données. L’issue d’intérêt était la mortalité à l’hôpital.
RÉSULTATS: Pendant la période de l’étude, un total de 11 300 patients atteints d’IAM a été repéré, dont 707 cas compliqués par un CC, pour une incidence d’IAM+CC de 6,3 %. Le taux de mortalité global des patients atteints d’IAM+CC était de 60,1 %. L’analyse de régression multivariée a permis d’établir que le fait d’avoir plus de 65 ans (RR 2,0; 95 % IC 1,4 à 2,9) et de souffrir d’insuffisance rénale (RR 2,1; 95 % IC 1,4 à 3,2) était un prédicteur indépendant de mortalité, tandis que l’accès à des soins cardiaques effractifs, défini comme une hospitalisation ou un transfert au seul centre apte à procéder à des cathétérismes cardiaques (à Halifax, en Nouvelle-Écosse), constituait un prédicteur indépendant de survie (RR 0,4; 95 % IC 0,3 à 0,5). L’accès à des soins cardiaques effractifs s’est limité à 414 patients (59 %), dont 250 (35 %) ont subi un cathétérisme cardiaque.
CONCLUSIONS: L’hospitalisation dans un centre de soins tertiaires capable d’offrir des soins effractifs s’associait de manière indépendante à une amélioration de la survie, tandis que le fait d’être âgé et de souffrir d’insuffisance rénale s’associait au décès chez les patients atteints d’IAM et de CC.
Figures
Similar articles
-
Where you Live in Nova Scotia Can Significantly Impact Your Access to Lifesaving Cardiac Care: Access to Invasive Care Influences Survival.Can J Cardiol. 2018 Feb;34(2):202-208. doi: 10.1016/j.cjca.2017.11.021. Can J Cardiol. 2018. PMID: 29407010
-
Changing practice patterns in the management of acute myocardial infarction complicated by cardiogenic shock: elderly compared with younger patients.Can J Cardiol. 1998 Jul;14(7):923-30. Can J Cardiol. 1998. PMID: 9706277
-
Trends in mechanical circulatory support use and hospital mortality among patients with acute myocardial infarction and non-infarction related cardiogenic shock in the United States.Clin Res Cardiol. 2018 Apr;107(4):287-303. doi: 10.1007/s00392-017-1182-2. Epub 2017 Nov 13. Clin Res Cardiol. 2018. PMID: 29134345
-
Acute myocardial infarction complicated by cardiogenic shock: role of mechanical circulatory support.Expert Rev Cardiovasc Ther. 2008 Oct;6(9):1223-35. doi: 10.1586/14779072.6.9.1223. Expert Rev Cardiovasc Ther. 2008. PMID: 18939910 Review.
-
Acute Myocardial Infarction and Cardiogenic Shock Interventional Approach to Management in the Cardiac Catheterization Laboratories.Curr Cardiol Rev. 2022;18(2):e251121198293. doi: 10.2174/1573403X17666211125090929. Curr Cardiol Rev. 2022. PMID: 34823461 Free PMC article. Review.
Cited by
-
Implementation of a Multidisciplinary Cardiogenic Shock Team in a Nonacademic Canadian Heart Centre: An Implementation Study.CJC Open. 2024 Nov 17;7(2):231-238. doi: 10.1016/j.cjco.2024.11.007. eCollection 2025 Feb. CJC Open. 2024. PMID: 40060208 Free PMC article.
-
Risk factors for cardiogenic shock incidence and mortality after acute myocardial infarction: a systematic review and meta-analysis.Commun Med (Lond). 2025 May 27;5(1):200. doi: 10.1038/s43856-025-00874-y. Commun Med (Lond). 2025. PMID: 40425745 Free PMC article.
References
-
- Goldberg RJ, Samad NA, Yarzebski J, Gurwitz J, Bigelow C, Gore JM. Temporal trends in cardiogenic shock complicating acute myocardial infarction. N Engl J Med. 1999;340:1162–8. - PubMed
-
- Goldberg RJ, Gore JM, Thompson CA, Gurwitz JH. Recent magnitude of and temporal trends (1994–1997) in the incidence and hospital death rates of cardiogenic shock complicating acute myocardial infarction: The second national registry of myocardial infarction. Am Heart J. 2001;141:65–72. - PubMed
-
- Gorge G, Haude M, Baumgart D, et al. [Therapy of cardiogenic shock in acute myocardial infarct. ] Herz. 1994;19:360–70. - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341:625–34. - PubMed
-
- Hochman JS. Cardiogenic shock complicating acute myocardial infarction: Expanding the paradigm. Circulation. 2003;107:2998–3002. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
