

Internal plate fixation of fractures: short history and recent developments
- PMID: 16568382
- PMCID: PMC2780616
- DOI: 10.1007/s00776-005-0984-7
Internal plate fixation of fractures: short history and recent developments
Abstract
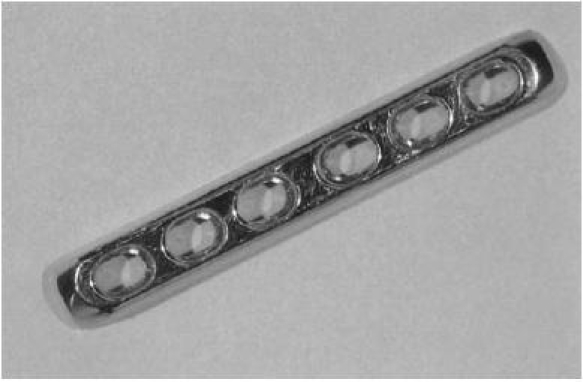
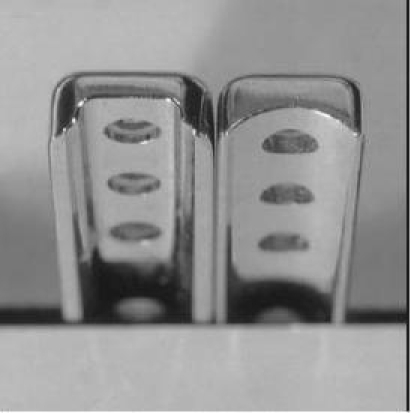
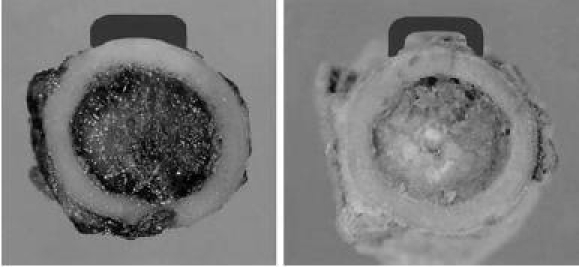
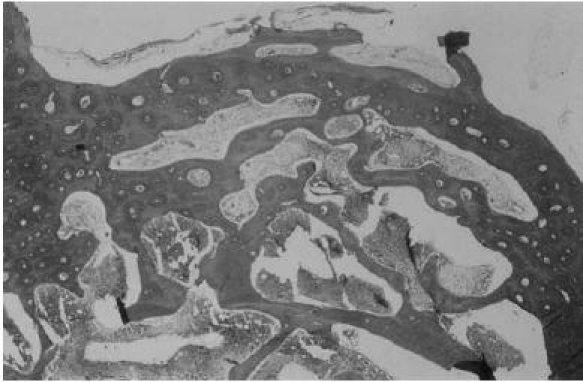
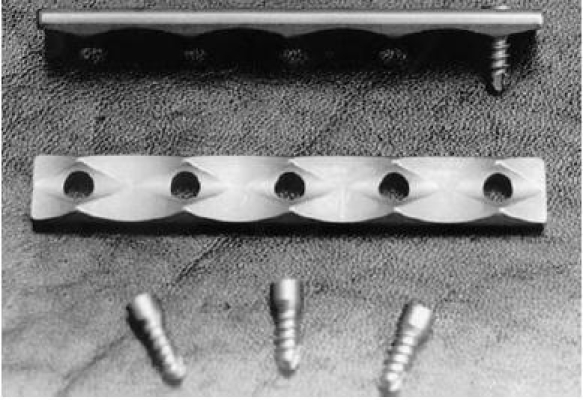
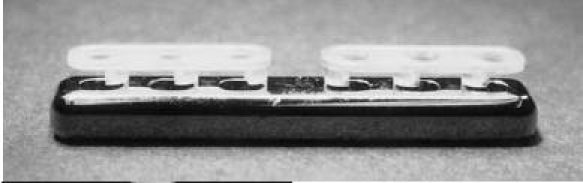
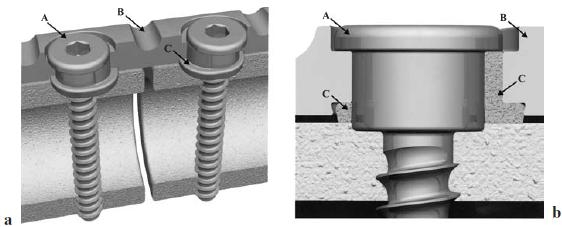
Metal plates for internal fixation of fractures have been used for more than 100 years. Although initial shortcomings such as corrosion and insufficient strength have been overcome, more recent designs have not solved all problems. Further research is needed to develop a plate that accelerates fracture healing while not interfering with bone physiology. The introduction of rigid plates had by far the greatest impact on plate fixation of fractures. However, it led to cortical porosis, delayed bridging, and refractures after plate removal. These unwarranted effects were said to be caused by bone-plate contact interfering with cortical perfusion. Consequently, further plate modifications aimed to reduce this contact area to minimize necrosis and subsequent porosis. The advocates of limited-contact plates have not published measurements of the contact area or proof of the temporary nature of the porosis. Moreover, clinical studies of newer plate types have failed to show a superior outcome. Histomor-phometric measurements of the cortex showed no difference in the extent of necrosis under plates having different contact areas. Necrosis was predominant in the periosteal cortical half, whereas porosis occurred mostly in the endosteal cortical half. No positive correlation was found between either. The scientific evidence to date strongly suggests that bone loss is caused by stress shielding and not interference with cortical perfusion secondary to bone-plate contact. Consequently, an axially compressible plate (ACP) incorporating polylactide (PLA) inserts press-fit around screw holes was designed. The bioresorbable inserts should allow for (1) increased micromotion in the axial plane to promote healing during the union phase and (2) gradual degradation over time to decrease stress shielding during the remodeling phase. Results of ongoing experimental results are encouraging. Only plates allowing dynamic compression in the axial plane can lead to a revolution in fracture fixation.
Figures





Similar articles
-
Biomechanical and histological evaluation of the application of biodegradable poly-L-lactic cushion to the plate internal fixation for bone fracture healing.Clin Biomech (Bristol). 2008;23 Suppl 1:S7-S16. doi: 10.1016/j.clinbiomech.2008.01.005. Epub 2008 Mar 4. Clin Biomech (Bristol). 2008. PMID: 18291564
-
Long-term effects of plate osteosynthesis: comparison of four different plates.Injury. 2000 May;31 Suppl 2:S-B51-62. doi: 10.1016/s0020-1383(00)80043-1. Injury. 2000. PMID: 10853761
-
Cortical bone perfusion in plated fractured sheep tibiae.J Orthop Res. 1995 Sep;13(5):715-24. doi: 10.1002/jor.1100130511. J Orthop Res. 1995. PMID: 7472750
-
Biomechanical and biological aspects of defect treatment in fractures using helical plates.Acta Chir Orthop Traumatol Cech. 2014;81(4):267-71. Acta Chir Orthop Traumatol Cech. 2014. PMID: 25137496 Review.
-
Bioresorbable fracture fixation in orthopedics: a comprehensive review. Part I. Basic science and preclinical studies.Am J Orthop (Belle Mead NJ). 1997 Oct;26(10):665-71. Am J Orthop (Belle Mead NJ). 1997. PMID: 9349887 Review.
Cited by
-
A Novel Shape Memory Plate Osteosynthesis for Noninvasive Modulation of Fixation Stiffness in a Rabbit Tibia Osteotomy Model.Biomed Res Int. 2015;2015:652940. doi: 10.1155/2015/652940. Epub 2015 Jun 8. Biomed Res Int. 2015. PMID: 26167493 Free PMC article.
-
DLS 5.0--the biomechanical effects of dynamic locking screws.PLoS One. 2014 Apr 10;9(4):e91933. doi: 10.1371/journal.pone.0091933. eCollection 2014. PLoS One. 2014. PMID: 24722267 Free PMC article.
-
Influence of the osteosynthesis plate on ultrasound propagation in the bone.Acta Ortop Bras. 2014;22(5):269-74. doi: 10.1590/1413-78522014220500733. Acta Ortop Bras. 2014. PMID: 25328436 Free PMC article.
-
Implant Removal Due to Infection After Open Reduction and Internal Fixation: Trends and Predictors.Arch Bone Jt Surg. 2022 Jun;10(6):514-524. doi: 10.22038/ABJS.2021.53838.2688. Arch Bone Jt Surg. 2022. PMID: 35928909 Free PMC article.
-
Hybrid fracture fixation systems developed for orthopaedic applications: A general review.J Orthop Translat. 2018 Jul 21;16:1-13. doi: 10.1016/j.jot.2018.06.006. eCollection 2019 Jan. J Orthop Translat. 2018. PMID: 30723676 Free PMC article. Review.
References
-
- Lambotte A. Technique et indication des prothèses dans le traitement des fractures. Presse Med. 1909;17:321.
-
- Sherman WO. Vanadium steel bone plates and screws. Surg Gynecol Obstet. 1912;14:629–34.
-
- Eggers GWN. Internal contact splint. J Bone Joint Surg Am. 1948;30:40–52. - PubMed
-
- Danis R. Théorie et pratique de l’ostéosynthèse. Paris: Masson; 1949.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
