

Advances and challenges in predicting the impact of lymphatic filariasis elimination programmes by mathematical modelling
- PMID: 16569234
- PMCID: PMC1448203
- DOI: 10.1186/1475-2883-5-5
Advances and challenges in predicting the impact of lymphatic filariasis elimination programmes by mathematical modelling
Abstract
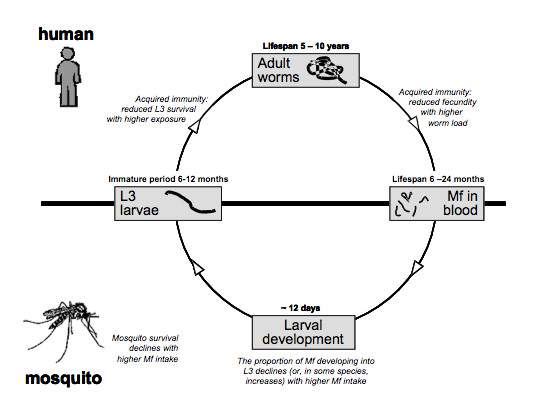
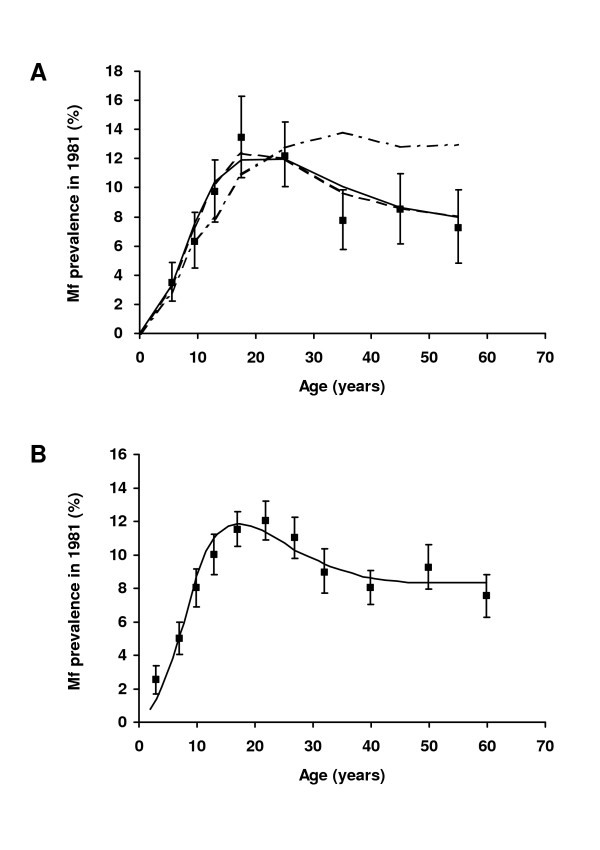
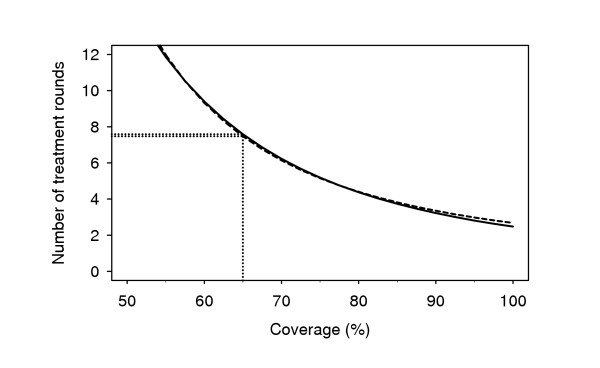
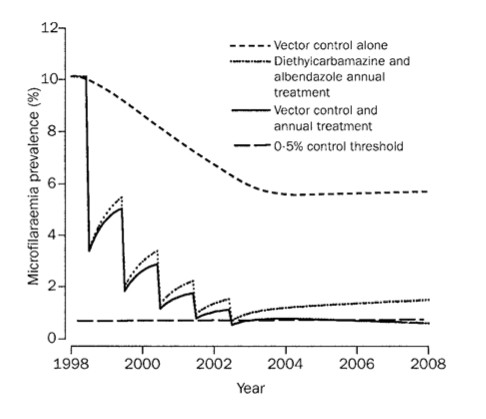
Mathematical simulation models for transmission and control of lymphatic filariasis are useful tools for studying the prospects of lymphatic filariasis elimination. Two simulation models are currently being used. The first, EPIFIL, is a population-based, deterministic model that simulates average trends in infection intensity over time. The second, LYMFASIM, is an individual-based, stochastic model that simulates acquisition and loss of infection for each individual in the simulated population, taking account of individual characteristics. For settings like Pondicherry (India), where Wuchereria bancrofti infection is transmitted by Culex quinquefasciatus, the models give similar predictions of the coverage and number of treatment rounds required to bring microfilaraemia prevalence below a level of 0.5%. Nevertheless, published estimates of the duration of mass treatment required for elimination differed, due to the use of different indicators for elimination (EPIFIL: microfilaraemia prevalence < 0.5% after the last treatment; LYMFASIM: reduction of microfilaraemia prevalence to zero, within 40 years after the start of mass treatment). The two main challenges for future modelling work are: 1) quantification and validation of the models for other regions, for investigation of elimination prospects in situations with other vector-parasite combinations and endemicity levels than in Pondicherry; 2) application of the models to address a range of programmatic issues related to the monitoring and evaluation of ongoing control programmes. The models' usefulness could be enhanced by several extensions; inclusion of different diagnostic tests and natural history of disease in the models is of particular relevance.
Figures
Similar articles
-
Mathematical modelling of lymphatic filariasis elimination programmes in India: required duration of mass drug administration and post-treatment level of infection indicators.Parasit Vectors. 2016 Sep 13;9(1):501. doi: 10.1186/s13071-016-1768-y. Parasit Vectors. 2016. PMID: 27624157 Free PMC article.
-
Modelling lymphatic filariasis transmission and control: modelling frameworks, lessons learned and future directions.Adv Parasitol. 2015 Mar;87:249-91. doi: 10.1016/bs.apar.2014.12.005. Epub 2015 Feb 13. Adv Parasitol. 2015. PMID: 25765197 Review.
-
Mathematical models for lymphatic filariasis transmission and control: Challenges and prospects.Parasit Vectors. 2008 Feb 12;1(1):2. doi: 10.1186/1756-3305-1-2. Parasit Vectors. 2008. PMID: 18275593 Free PMC article.
-
Prospects for elimination of bancroftian filariasis by mass drug treatment in Pondicherry, India: a simulation study.J Infect Dis. 2003 Nov 1;188(9):1371-81. doi: 10.1086/378354. Epub 2003 Oct 31. J Infect Dis. 2003. PMID: 14593597
-
Mathematical modelling and the control of lymphatic filariasis.Lancet Infect Dis. 2004 Apr;4(4):223-34. doi: 10.1016/S1473-3099(04)00973-9. Lancet Infect Dis. 2004. PMID: 15050941 Review.
Cited by
-
Risk of Recrudescence of Lymphatic Filariasis after Post-MDA Surveillance in Brugia malayi Endemic Belitung District, Indonesia.Korean J Parasitol. 2020 Dec;58(6):627-634. doi: 10.3347/kjp.2020.58.6.627. Epub 2020 Dec 29. Korean J Parasitol. 2020. PMID: 33412766 Free PMC article.
-
The effect of compliance on the impact of mass drug administration for elimination of lymphatic filariasis in Egypt.Am J Trop Med Hyg. 2007 Dec;77(6):1069-73. Am J Trop Med Hyg. 2007. PMID: 18165524 Free PMC article.
-
Preventive chemotherapy in human helminthiasis: theoretical and operational aspects.Trans R Soc Trop Med Hyg. 2011 Dec;105(12):683-93. doi: 10.1016/j.trstmh.2011.08.013. Epub 2011 Oct 29. Trans R Soc Trop Med Hyg. 2011. PMID: 22040463 Free PMC article.
-
Diurnally subperiodic filariasis in India-prospects of elimination: precept to action?Parasitol Res. 2011 Jul;109(1):1-8. doi: 10.1007/s00436-011-2252-4. Epub 2011 Feb 1. Parasitol Res. 2011. PMID: 21286754 Review.
-
What Is Needed to Eradicate Lymphatic Filariasis? A Model-Based Assessment on the Impact of Scaling Up Mass Drug Administration Programs.PLoS Negl Trop Dis. 2015 Oct 9;9(10):e0004147. doi: 10.1371/journal.pntd.0004147. eCollection 2015. PLoS Negl Trop Dis. 2015. PMID: 26451729 Free PMC article.
References
-
- World Health Organization Global Programme to Eliminate Lymphatic Filariasis - Progress report for 2004. Wkly Epidemiol Rec. 2005;80:202–212. - PubMed
-
- Schlemper BRJ, Steindel M, Grisard EC, Carvalho-Pinto CJ, Bernardini OJ, de Castilho CV, Rosa G, Kilian S, Guarneri AA, Rocha A, Medeiros Z, Ferreira Neto JA. Elimination of bancroftian filariasis (Wuchereria bancrofti) in Santa Catarina state, Brazil. Trop Med Int Health. 2000;5:848–854. doi: 10.1046/j.1365-3156.2000.00661.x. - DOI - PubMed
-
- VCRC . Annual report 2003. , Vector Control Research Centre, Pondicherry, India.; 2003.
LinkOut - more resources
Full Text Sources
