

Magnetic resonance imaging in psoriatic arthritis: a review of the literature
- PMID: 16569257
- PMCID: PMC1526607
- DOI: 10.1186/ar1934
Magnetic resonance imaging in psoriatic arthritis: a review of the literature
Abstract
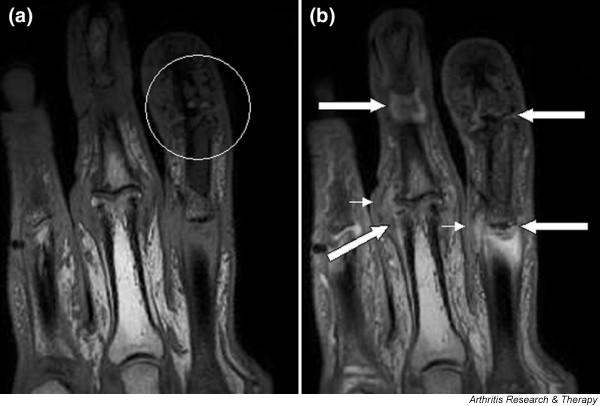
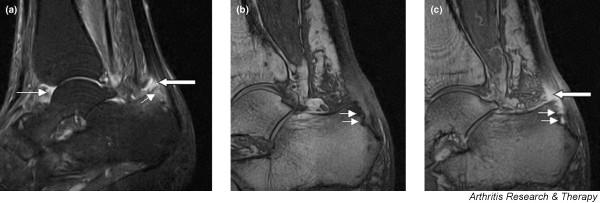
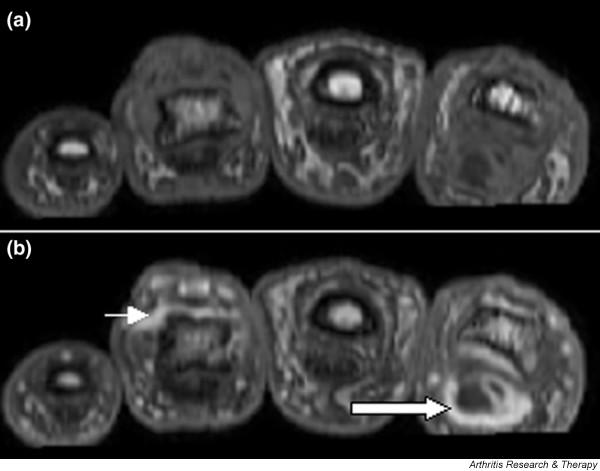
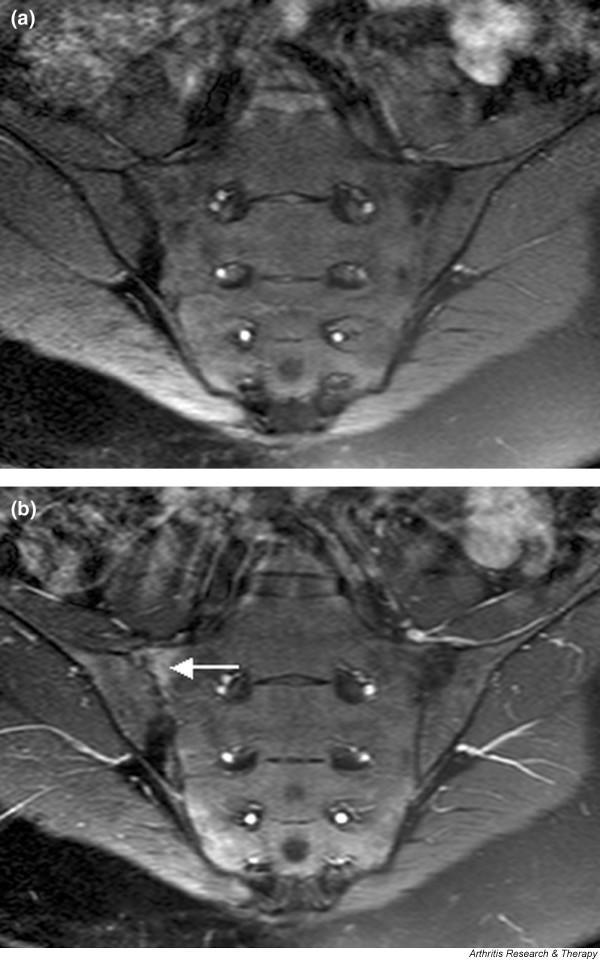
Psoriatic arthritis is a diverse condition that may be characterized by peripheral inflammatory arthritis, axial involvement, dactylitis and enthesitis. Magnetic resonance imaging (MRI) allows visualization of soft tissue, articular and entheseal lesions, and provides a unique picture of the disease process that cannot be gained using other imaging modalities. This review focuses on the literature on MRI in psoriatic arthritis published from 1996 to July 2005. The MRI features discussed include synovitis, tendonitis, dactylitis, bone oedema, bone erosions, soft tissue oedema, spondylitis/sacroiliitis and subclinical arthropathy. Comparisons have been drawn with the more extensive literature describing the MRI features of rheumatoid arthritis and ankylosing spondylitis.
Figures


References
-
- Antoni C, Dechant C, Lorenz PDH, Wendler J, Ogilvie A, Lueftl M, Kalden-Nemeth D, Kalden JR, Manger B. Open-label study of infliximab treatment for psoriatic arthritis: clinical and magnetic resonance imaging measurements of reduction of inflammation. Arthritis Care Res. 2002;47:506–512. doi: 10.1002/art.10671. - DOI - PubMed
-
- Backhaus M, Kamradt T, Sandrock D, Loreck D, Fritz J, Wolf KJ, Raber H, Hamm B, Burmester GR, Bollow M. Arthritis of the finger joints. A comprehensive approach comparing conventional radiography, scintigraphy, ultrasound and contrast-enhanced MRI. Arthritis Rheum. 1999;42:1232–1234. doi: 10.1002/1529-0131(199906)42:6<1232::AID-ANR21>3.0.CO;2-3. - DOI - PubMed
-
- Bollow M, Braun J, Hamm B, Eggens U, Schilling A, Konig H, Wolf KJ. Early sacroiliitis in patients with spondyloarthropathy: evaluation with dynamic gadolinium-enhanced MR imaging. Radiology. 1995;194:529–536. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
