

Prevalence of sputum smear-positive tuberculosis in a rural area in Bangladesh
- PMID: 16569271
- PMCID: PMC2870495
- DOI: 10.1017/S0950268806006108
Prevalence of sputum smear-positive tuberculosis in a rural area in Bangladesh
Abstract
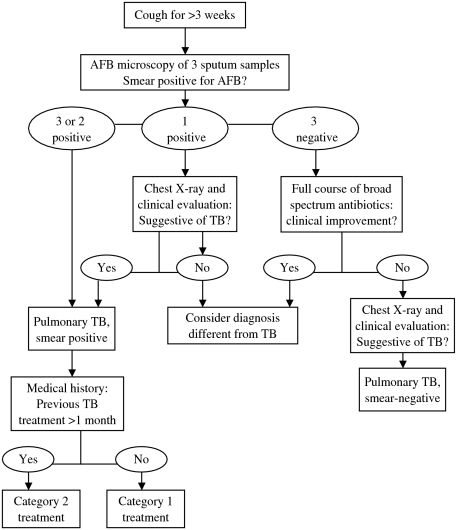
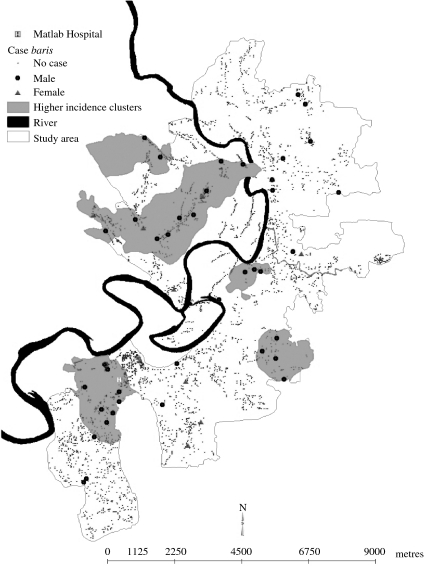
The objective of the study was to determine the prevalence of smear-positive tuberculosis (TB) in a rural area in Bangladesh at Matlab. A TB surveillance system was established among 106,000 people in rural Bangladesh at Matlab. Trained field workers interviewed all persons aged > or = 15 years to detect suspected cases of TB (cough > 21 days) and sputum specimens of suspected cases were examined for acid-fast bacilli (AFB). Of 59,395 persons interviewed, 4235 (7.1%) had a cough for > 21 days. Sputum specimens were examined for AFB from 3834 persons, 52 (1.4%) of them were positive for AFB. The prevalence of chronic cough and sputum positivity were significantly higher among males compared to females (P < 0.001). The population-based prevalence rate of smear-positive TB cases was 95/100,000 among persons aged > or = 15 years. Cases of TB clustered geographically (relative risk 5.53, 95% CI 3.19-9.59). The high burden of TB among rural population warrants appropriate measures to control TB in Bangladesh. The higher prevalence of persistent cough and AFB-positive sputum among males need further exploration. Factors responsible for higher prevalence of TB in clusters should be investigated.
Figures
References
-
- World Health Organization Geneva: 2003. . Global tuberculosis control: surveillance, planning, financing. WHO Report 2003 (WHO/CDS/TB/2003.316). : WHO,
-
- World Health Organization New Delhi, India: 2003. . Tuberculosis control in the south-east Asia region: the regional report 2003 (SEA/TB/260). : WHO,
-
- Director General Health Services (DGHS) Dhaka: 1989. . Report on the national prevalence survey on tuberculosis in Bangladesh, 1987–88. : Ministry of Health and Family Welfare, Government of Bangladesh,
-
- Kumaresan JA, Raviglione MC, Murray CJL, Murray CLJ, Lopez AD. Global Health Statistics: global burden of disease and injury series. Vol. 2. Boston, MA: Harvard University Press; 1996. Tuberculosis; pp. 142–147. , vol. : pp.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
