

Roll rotation cues influence roll tilt perception assayed using a somatosensory technique
- PMID: 16571732
- PMCID: PMC1661663
- DOI: 10.1152/jn.01163.2005
Roll rotation cues influence roll tilt perception assayed using a somatosensory technique
Abstract
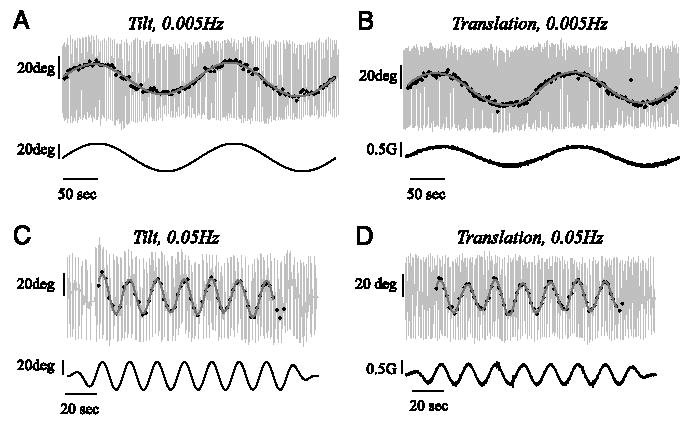
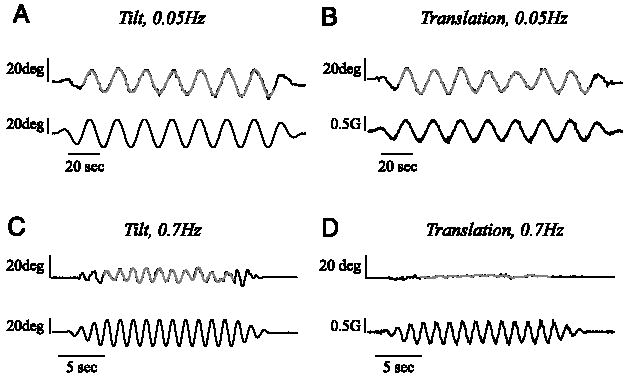
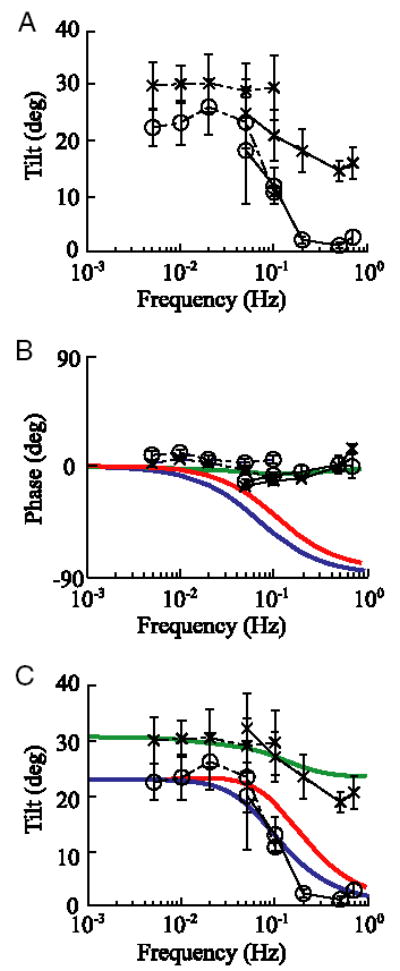
We investigated how the nervous system processes ambiguous cues from the otolith organs by measuring roll tilt perception elicited by two motion paradigms. In one paradigm (tilt), eight subjects were sinusoidally tilted in roll with the axis of rotation near ear level. Stimulus frequencies ranged from 0.005 to 0.7 Hz, and the peak amplitude of tilt was 20 degrees . During this paradigm, subjects experienced a sinusoidal variation of interaural gravitational force with a peak of 0.34 g. The second motion paradigm (translation) was designed to yield the same sinusoidal variation in interaural force but did not include a roll canal cue. This was achieved by sinusoidally translating the subjects along their interaural axis. For the 0.7-Hz translation trial, the subjects were simply translated from side to side. A centrifuge was used for the 0.005- to 0.5-Hz translation trials; the subjects were rotated in yaw at 250 degrees /s for 5 min before initiating sinusoidal translations yielding an interaural otolith stimulus composed of both centrifugal and radial acceleration. Using a somatosensory task to measure roll tilt perception, we found substantial differences in tilt perception during the two motion paradigms. Because the primary difference between the two motion paradigms was the presence of roll canal cues during roll tilt trials, these perceptual differences suggest that canal cues influence tilt perception. Specifically, rotational cues provided by the semicircular canals help the CNS resolve ambiguous otolith cues during head tilt, yielding more accurate tilt perception.
Figures
Similar articles
-
Vestibular perception and action employ qualitatively different mechanisms. I. Frequency response of VOR and perceptual responses during Translation and Tilt.J Neurophysiol. 2005 Jul;94(1):186-98. doi: 10.1152/jn.00904.2004. Epub 2005 Feb 23. J Neurophysiol. 2005. PMID: 15728767
-
Vestibular perception and action employ qualitatively different mechanisms. II. VOR and perceptual responses during combined Tilt&Translation.J Neurophysiol. 2005 Jul;94(1):199-205. doi: 10.1152/jn.00905.2004. Epub 2005 Feb 23. J Neurophysiol. 2005. PMID: 15730979
-
Neural processing of gravito-inertial cues in humans. IV. Influence of visual rotational cues during roll optokinetic stimuli.J Neurophysiol. 2003 Jan;89(1):390-400. doi: 10.1152/jn.00513.2001. J Neurophysiol. 2003. PMID: 12522188
-
Rotation otolith tilt-translation reinterpretation (ROTTR) hypothesis: a new hypothesis to explain neurovestibular spaceflight adaptation.J Vestib Res. 2003;13(4-6):309-20. J Vestib Res. 2003. PMID: 15096674 Review.
-
The interaction of otolith and proprioceptive information in the perception of verticality. The effects of labyrinthine and CNS disease.Ann N Y Acad Sci. 1999 May 28;871:324-33. doi: 10.1111/j.1749-6632.1999.tb09195.x. Ann N Y Acad Sci. 1999. PMID: 10372082 Review.
Cited by
-
The time constant of the somatogravic illusion.Exp Brain Res. 2013 Feb;224(3):313-21. doi: 10.1007/s00221-012-3313-3. Epub 2012 Nov 4. Exp Brain Res. 2013. PMID: 23124839
-
Phase-linking and the perceived motion during off-vertical axis rotation.Biol Cybern. 2010 Jan;102(1):9-29. doi: 10.1007/s00422-009-0347-0. Epub 2009 Nov 24. Biol Cybern. 2010. PMID: 19937069 Free PMC article.
-
Amplification of vibration induced nystagmus in patients with peripheral vestibular loss by head tilt.Front Neurol. 2024 Oct 16;15:1420699. doi: 10.3389/fneur.2024.1420699. eCollection 2024. Front Neurol. 2024. PMID: 39479011 Free PMC article.
-
Modeling human perception of orientation in altered gravity.Front Syst Neurosci. 2015 May 5;9:68. doi: 10.3389/fnsys.2015.00068. eCollection 2015. Front Syst Neurosci. 2015. PMID: 25999822 Free PMC article.
-
Central Integration of Canal and Otolith Signals is Abnormal in Vestibular Migraine.Front Neurol. 2014 Nov 10;5:233. doi: 10.3389/fneur.2014.00233. eCollection 2014. Front Neurol. 2014. PMID: 25426098 Free PMC article. Review.
References
-
- Benson AJ, Spencer MB, Stott JR. Thresholds for the detection of the direction of whole-body, linear movement in the horizontal plane. Aviat Space Environ Med. 1986;57:1088–1096. - PubMed
-
- Clark B, Graybiel A. Contributing factors in the perception of the oculogravic illusion. Am J Psychol. 1963;76:18–27. - PubMed
-
- Clement G, Maciel F, Deguine O. Perception of tilt and ocular torsion of normal human subjects during eccentric rotation. Otol Neurotol. 2002;23:958–966. - PubMed
-
- Clement G, Moore ST, Raphan T, Cohen B. Perception of tilt (somatogravic illusion) in response to sustained linear acceleration during space flight. Exp Brain Res. 2001;138:410–418. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources