

Hyperkalemia revisited
Abstract
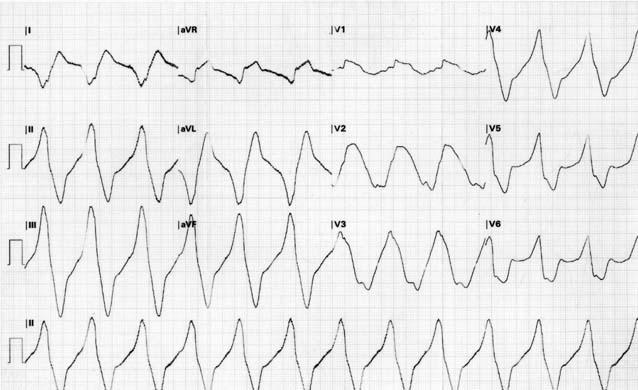
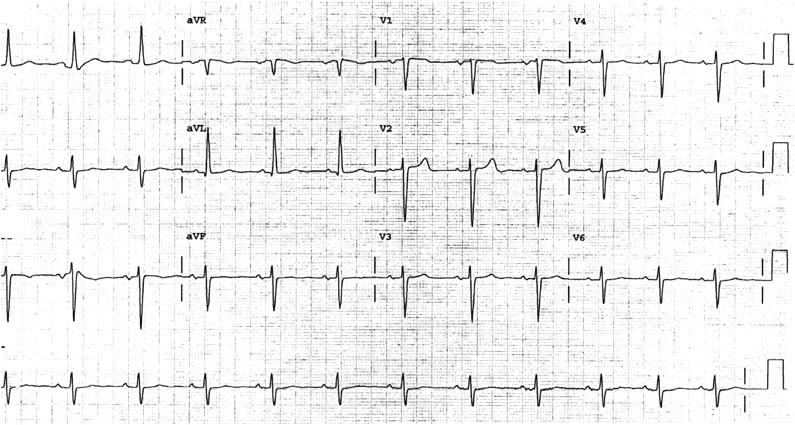
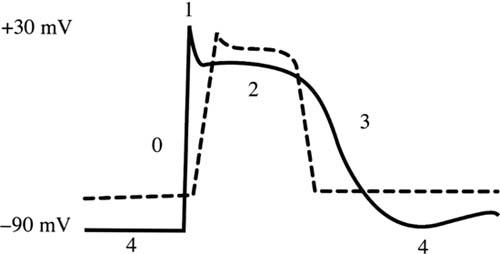
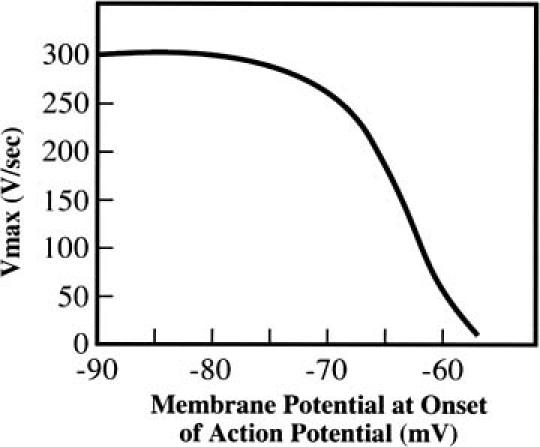
Hyperkalemia is a common clinical condition that can induce deadly cardiac arrhythmias. Electrocardiographic manifestations of hyperkalemia vary from the classic sine-wave rhythm, which occurs in severe hyperkalemia, to nonspecific repolarization abnormalities seen with mild elevations of serum potassium. We present a case of hyperkalemia, initially diagnosed as ventricular tachycardia, to demonstrate how difficult hyperkalemia can be to diagnose. An in-depth review of hyperkalemia is presented, examining the electrophysiologic and electrocardiographic changes that occur as serum potassium levels increase. The treatment for hyperkalemia is then discussed, with an emphasis on the mechanisms by which each intervention lowers serum potassium levels. An extensive literature review has been performed to present a comprehensive review of the causes and treatment of hyperkalemia.
Figures
References
-
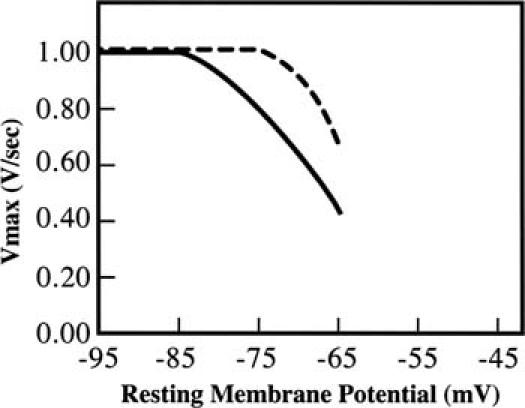
- Gettes LS. Effects of ionic changes on impulse propagation. In: Rosen MR, Janse MJ, Wit AL, editors. Cardiac electrophysiology: a textbook. Mount Kisco (NY): Futura Publishing Co; 1990. p. 459–80.
-
- Acker CG, Johnson JP, Palevsky PM, Greenberg A. Hyperkalemia in hospitalized patients: causes, adequacy of treatment, and results of an attempt to improve physician com-pliance with published therapy guidelines. Arch Intern Med 1998;158:917–24. - PubMed
-
- Tarail R. Relation of abnormalities in concentration of serum potassium to electrocardiographic disturbances. Am J Med 1948;5:828–37. - PubMed
-
- Szerlip HM, Weiss J, Singer I. Profound hyperkalemia without electrocardiographic manifestations. Am J Kidney Dis 1986;7:461–5. - PubMed
-
- Martinez-Vea A, Bardaji A, Garcia C, Oliver JA. Severe hyperkalemia with minimal electrocardiographic manifestations: a report of seven cases. J Electrocardiol 1999;32:45–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources