

Epidemiology of HPV 16 and cervical cancer in Finland and the potential impact of vaccination: mathematical modelling analyses
- PMID: 16573364
- PMCID: PMC1434486
- DOI: 10.1371/journal.pmed.0030138
Epidemiology of HPV 16 and cervical cancer in Finland and the potential impact of vaccination: mathematical modelling analyses
Abstract
Background: Candidate human papillomavirus (HPV) vaccines have demonstrated almost 90%-100% efficacy in preventing persistent, type-specific HPV infection over 18 mo in clinical trials. If these vaccines go on to demonstrate prevention of precancerous lesions in phase III clinical trials, they will be licensed for public use in the near future. How these vaccines will be used in countries with national cervical cancer screening programmes is an important question.
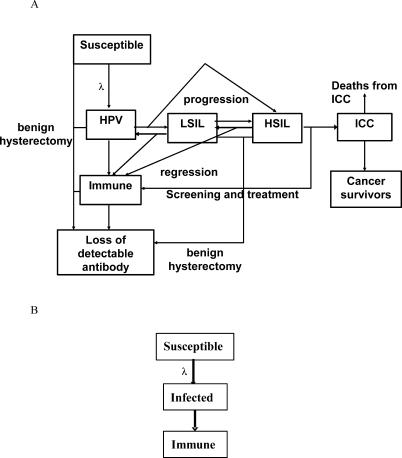
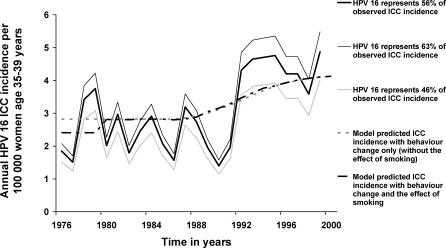
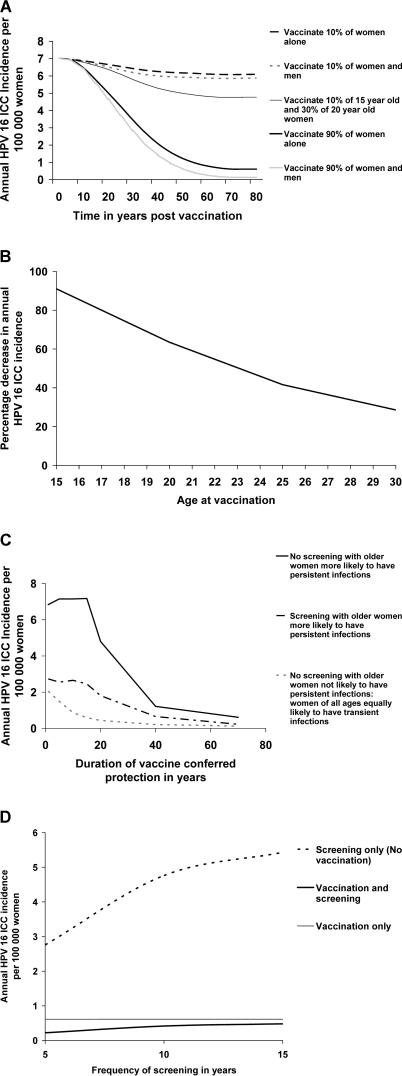
Methods and findings: We developed a transmission model of HPV 16 infection and progression to cervical cancer and calibrated it to Finnish HPV 16 seroprevalence over time. The model was used to estimate the transmission probability of the virus, to look at the effect of changes in patterns of sexual behaviour and smoking on age-specific trends in cancer incidence, and to explore the impact of HPV 16 vaccination. We estimated a high per-partnership transmission probability of HPV 16, of 0.6. The modelling analyses showed that changes in sexual behaviour and smoking accounted, in part, for the increase seen in cervical cancer incidence in 35- to 39-y-old women from 1990 to 1999. At both low (10% in opportunistic immunisation) and high (90% in a national immunisation programme) coverage of the adolescent population, vaccinating women and men had little benefit over vaccinating women alone. We estimate that vaccinating 90% of young women before sexual debut has the potential to decrease HPV type-specific (e.g., type 16) cervical cancer incidence by 91%. If older women are more likely to have persistent infections and progress to cancer, then vaccination with a duration of protection of less than 15 y could result in an older susceptible cohort and no decrease in cancer incidence. While vaccination has the potential to significantly reduce type-specific cancer incidence, its combination with screening further improves cancer prevention.
Conclusions: HPV vaccination has the potential to significantly decrease HPV type-specific cervical cancer incidence. High vaccine coverage of women alone, sustained over many decades, with a long duration of vaccine-conferred protection, would have the greatest impact on type-specific cancer incidence. This level of coverage could be achieved through national coordinated programmes, with surveillance to detect cancers caused by nonvaccine oncogenic HPV types.
Conflict of interest statement
Figures
Comment in
-
Mathematical model of HPV provides insight into impacts of risk factors and vaccine.PLoS Med. 2006 May;3(5):e164. doi: 10.1371/journal.pmed.0030164. Epub 2006 Apr 4. PLoS Med. 2006. PMID: 16573363 Free PMC article.
References
-
- Munoz N, Bosch FX, de Sanjose S, Herrero R, Castellsague X, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348:518–527. - PubMed
-
- Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189:12–19. - PubMed
-
- zur Hausen H. Papillomaviruses causing cancer: Evasion from host-cell control in early events in carcinogenesis. J Natl Cancer Inst. 2000;92:690–698. - PubMed
-
- Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. 1998;338:423–428. - PubMed
