

Descriptive epidemiology and prior healthcare utilization of patients in the Spine Patient Outcomes Research Trial's (SPORT) three observational cohorts: disc herniation, spinal stenosis, and degenerative spondylolisthesis
- PMID: 16582855
- PMCID: PMC2775468
- DOI: 10.1097/01.brs.0000207473.09030.0d
Descriptive epidemiology and prior healthcare utilization of patients in the Spine Patient Outcomes Research Trial's (SPORT) three observational cohorts: disc herniation, spinal stenosis, and degenerative spondylolisthesis
Abstract
Study design: Prospective observational cohorts.
Objective: To describe sociodemographic and clinical features, and nonoperative (medical) resource utilization before enrollment, in patients who are candidates for surgical intervention for intervertebral disc herniation (IDH), spinal stenosis (SpS), and degenerative spondylolisthesis (DS) according to SPORT criteria.
Summary of background data: Intervertebral disc herniation, spinal stenosis, and degenerative spondylolisthesis with stenosis are the three most common diagnoses of low back and leg symptoms for which surgery is performed. There is a paucity of descriptive literature examining large patient cohorts for the relationships among baseline characteristics and medical resource utilization with these three diagnoses.
Methods: The Spine Patient Outcomes Research Trial (SPORT) conducts three randomized and three observational cohort studies of surgical and nonsurgical treatments for patients with IDH, SpS, and DS. Baseline data include demographic information, prior treatments received, and functional status measured by SF-36 and the Oswestry Disability Index (ODI-AAOS/Modems version). The data presented represent all 1,411 patients (743 IDH, 365 SpS, 303 DS) enrolled in the SPORT observational cohorts. Multiple logistic regression was used to generate independent predictors of utilization adjusted for sociodemographic variables, diagnosis, and duration of symptoms.
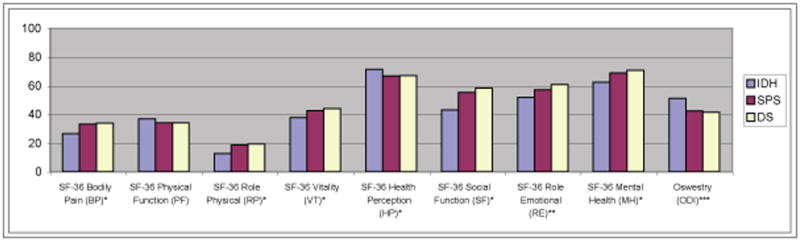
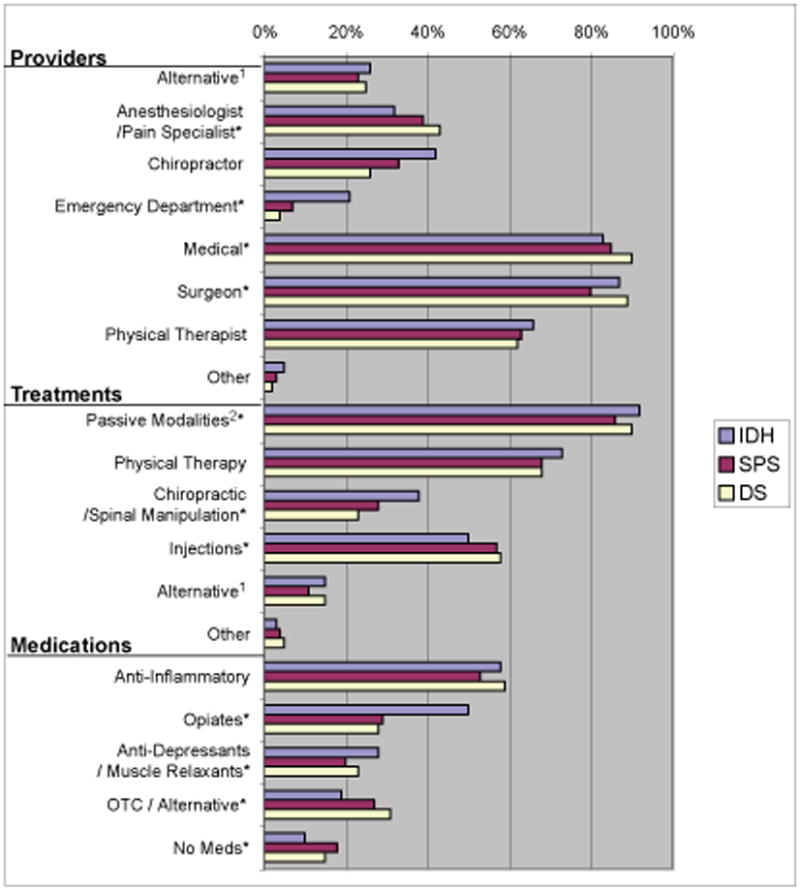
Results: The average age was 41 years for the IDH group, 64 years for the SpS group, and 66 years for the DS group. At enrollment, IDH patients presented with the most pain as reported on the SF-36 (BP 26.3 vs. 33.2 SpS and 33.8 DS) and were the most impaired (ODI 51 vs. 42.3 SpS and 41.5 DS). IDH patients used more chiropractic treatment (42% vs. 33% SpS and 26% DS), had more Emergency Department (ED) visits (21% vs. 7% SpS and 4% DS), and used more opiate analgesics (49% vs. 29% SpS and 27% DS). After adjusting for age, gender, diagnosis, education, race, duration of symptoms, and compensation, Medicaid patients used significantly more opiate analgesics (58% Medicaid vs. 41% no insurance, 42% employer, 33% Medicare, and 32% private) and had more ED visits compared with other insurance types (31% Medicaid vs. 22% no insurance, 16% employer, 3% Medicare, and 11% private).
Conclusion: IDH patients appear to have differences in sociodemographics, resource utilization, and functional impairment when compared with the SpS/DS patients. In addition, the differences in resource utilization for Medicaid patients may reflect differences in access to care. The data provided from these observational cohorts will serve as an important comparison to the SPORT randomized cohorts in the future.
Figures
References
-
- Cherkin DC, Deyo RA, Loeser JD, et al. An international comparison of back surgery rates. Spine. 1994;19(11):1201–6. - PubMed
-
- Ware JE., Jr SF-36 health survey update. Spine. 2000;25(24):3130–9. - PubMed
-
- Fairbank JC, Pynsent PB. The Oswestry Disability Index. Spine. 2000;25(22):2940–52. discussion 52. - PubMed
-
- Deyo RA, Weinstein JN. Low back pain. New England Journal of Medicine. 2001;344(5):363–70. - PubMed
-
- Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine. 1995;20(1):11–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
