

Amino-terminal pro-B-type natriuretic peptide and B-type natriuretic peptide: biomarkers for mortality in a large community-based cohort free of heart failure
- PMID: 16585413
- PMCID: PMC2647805
- DOI: 10.1161/01.HYP.0000216794.24161.8c
Amino-terminal pro-B-type natriuretic peptide and B-type natriuretic peptide: biomarkers for mortality in a large community-based cohort free of heart failure
Abstract
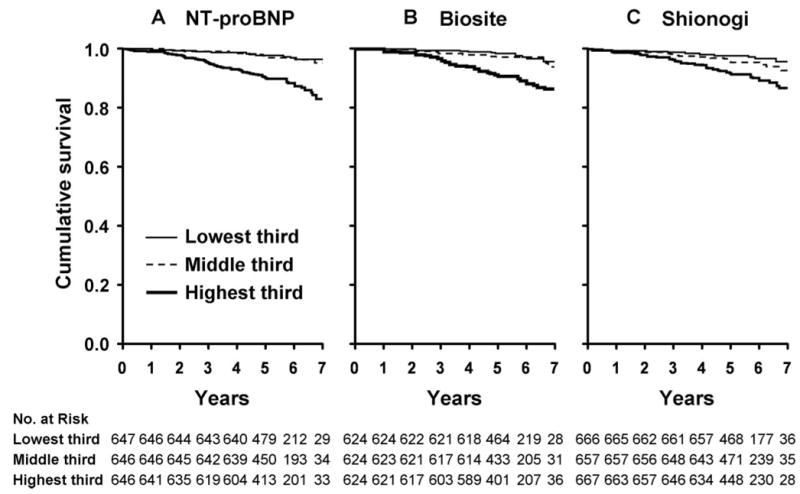
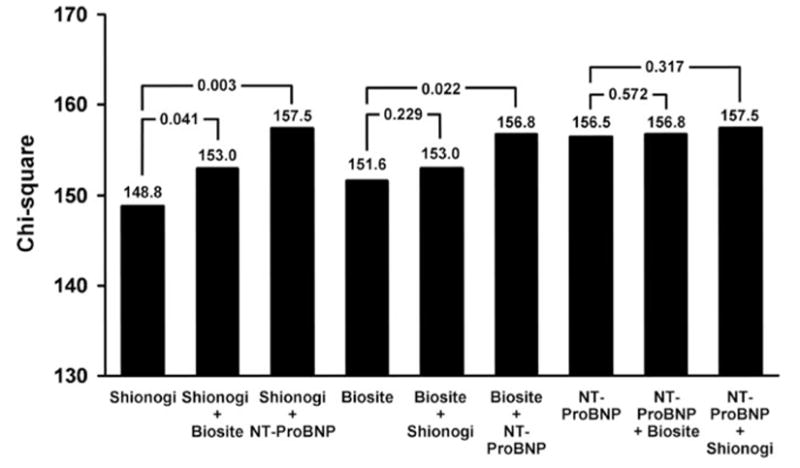
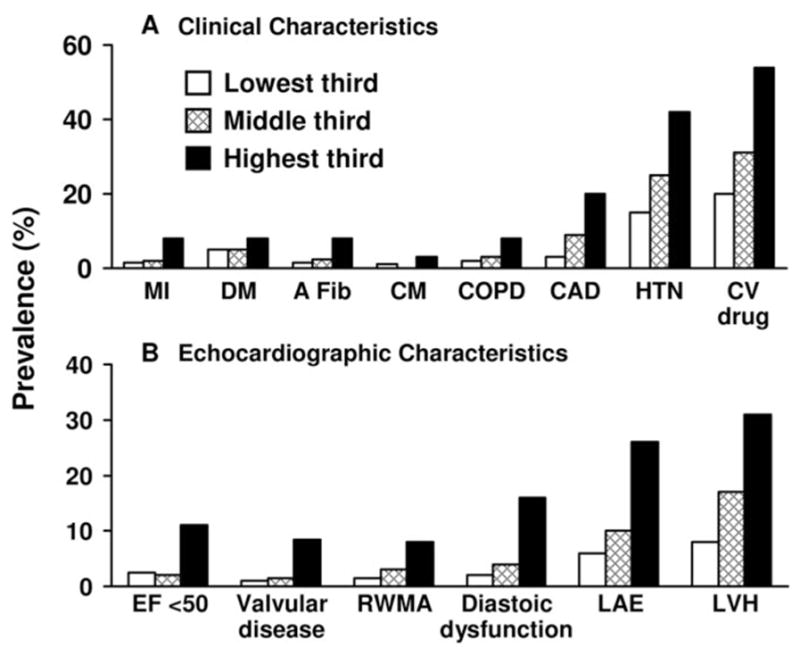
Recent studies report that, in the absence of heart failure and renal failure, plasma B-type natriuretic peptide (BNP) has prognostic value for mortality. We sought to confirm and extend these previous studies to assess BNP, measured by 3 distinct assays, as a biomarker for mortality in a strategy to enhance efforts at primary prevention and to better understand the clinical phenotype of such subjects at risk. We used a community-based cohort of 2042 subjects from Olmsted County, Minn, and individuals with heart or renal failure were excluded. BNP was assessed using 3 assays including Biosite and Shionogi for mature, biologically active BNP and the Roche assay for apparently nonbiologically active amino-terminal pro-BNP (NT-proBNP). Thorough echocardiographic and clinical data were recorded for all of the participants. Median follow-up for mortality was 5.6 years. BNP by all 3 of the assays was predictive of mortality. NT-proBNP and Biosite assays remained significant even after adjustment for traditional clinical risk factors and echocardiographic abnormalities including left ventricular hypertrophy and diastolic dysfunction. Echocardiography documented widespread structural changes in those with increasing BNP levels yet below levels observed in heart failure. We report in a large, well-characterized community-based cohort, free of heart failure, the first study to compare 3 distinct BNP assays as biomarkers for mortality in the same cohort. Our findings confirm the potential use of NT-proBNP and BNP biomarkers for future events and underscore that these peptides may also serve as biomarkers for underlying cardiac remodeling secondary to diverse cardiovascular disease entities.
Figures
References
-
- Heidenreich PA, Gubens MA, Fonarow GC, Konstam MA, Stevenson LW, Shekelle PG. Cost-effectiveness of screening with B-type natriuretic peptide to identify patients with reduced left ventricular ejection fraction. J Am Coll Cardiol. 2004;43:1019–1026. - PubMed
-
- Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, Omland T, Storrow AB, Abraham WT, Wu AH, Clopton P, Steg PG, Westheim A, Knudsen CW, Perez A, Kazanegra R, Herrmann HC, McCullough PA. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161–167. - PubMed
-
- McCullough PA, Nowak RM, McCord J, Hollander JE, Herrmann HC, Steg PG, Duc P, Westheim A, Omland T, Knudsen CW, Storrow AB, Abraham WT, Lamba S, Wu AH, Perez A, Clopton P, Krishnaswamy P, Kazanegra R, Maisel AS. B-type natriuretic peptide and clinical judgment in emergency diagnosis of heart failure: analysis from Breathing Not Properly (BNP) Multinational Study. Circulation. 2002;106:416–422. - PubMed
-
- Wang TJ, Larson MG, Levy D, Benjamin EJ, Leip EP, Omland T, Wolf PA, Vasan RS. Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N Engl J Med. 2004;350:655–663. - PubMed
-
- Kistorp C, Raymond I, Pedersen F, Gustafsson F, Faber J, Hildebrandt P. N-terminal pro-brain natriuretic peptide, c-reactive protein, and urinary albumin levels as predictors of mortality and cardiovascular events in older adults. JAMA. 2005;293:1609–1616. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
