

Therapy modifications in response to poorly controlled hypertension, dyslipidemia, and diabetes mellitus
- PMID: 16585661
- PMCID: PMC2577322
- DOI: 10.7326/0003-4819-144-7-200604040-00006
Therapy modifications in response to poorly controlled hypertension, dyslipidemia, and diabetes mellitus
Abstract
Background: Poorly controlled cardiovascular risk factors are common. Evaluating whether physicians respond appropriately to poor risk factor control in patients may better reflect quality of care than measuring proportions of patients whose conditions are controlled.
Objectives: To evaluate therapy modifications in response to poor control of hypertension, dyslipidemia, or diabetes in a large clinical population.
Design: Retrospective cohort study within an 18-month period in 2002 to 2003.
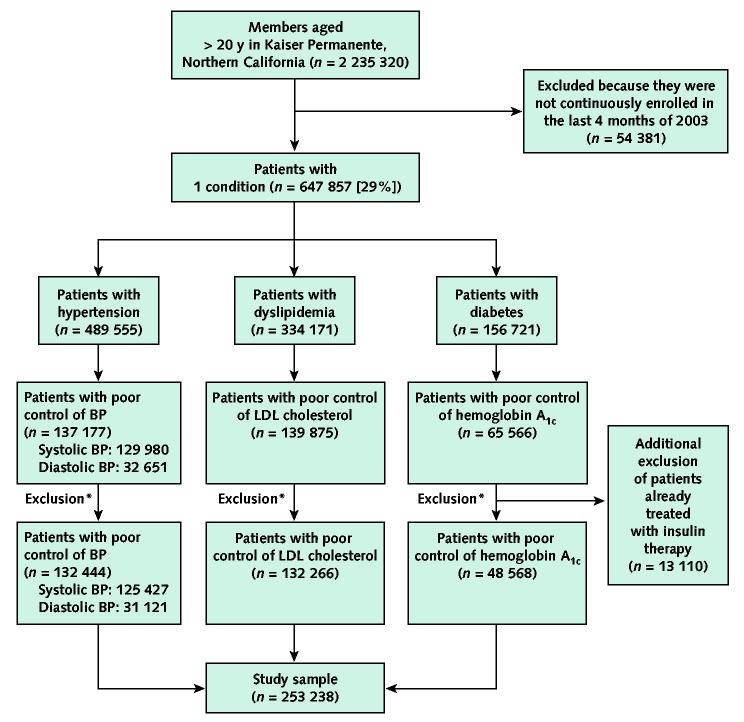
Setting: Kaiser Permanente of Northern California.
Patients: 253,238 adult members with poor control of 1 or more of these conditions.
Measurements: The authors assessed the proportion of patients with poor control who experienced a change in pharmacotherapy within 6 months, and they defined "appropriate care" as a therapy modification or return to control without therapy modification within 6 months.
Results: A total of 64% of patients experienced modifications in therapy for poorly controlled systolic blood pressure, 71% for poorly controlled diastolic blood pressure, 56% for poorly controlled low-density lipoprotein cholesterol level, and 66% for poorly controlled hemoglobin A1c level. Most frequent modifications were increases in number of drug classes (from 70% to 84%) and increased dosage (from 15% to 40%). An additional 7% to 11% of those with poorly controlled blood pressure, but only 3% to 4% of those with elevated low-density lipoprotein cholesterol level or hemoglobin A1c level, returned to control without therapy modification. Patients with more than 1 of the 3 conditions, higher baseline values, and target organ damage were more likely to receive "appropriate care."
Limitations: Patient preferences and suboptimal adherence to therapy were not measured and may explain some failures to act.
Conclusions: As an additional measure of the quality of care, measuring therapy modifications in response to poor control in a large population is feasible. Many patients with poorly controlled hypertension, dyslipidemia, or diabetes had their therapy modified and, thus, seemed to receive clinically "appropriate care" with this new quality measure.
Figures
Comment in
-
Improving the outcomes of metabolic conditions: managing momentum to overcome clinical inertia.Ann Intern Med. 2006 Apr 4;144(7):525-7. doi: 10.7326/0003-4819-144-7-200604040-00012. Ann Intern Med. 2006. PMID: 16585667 No abstract available.
-
Poorly controlled cardiovascular risk factors and ICD-9-CM codes.Ann Intern Med. 2006 Sep 5;145(5):394; author reply 394-5. doi: 10.7326/0003-4819-145-5-200609050-00019. Ann Intern Med. 2006. PMID: 16954367 No abstract available.
References
-
- MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7–22. [PMID: 12114036] - PubMed
-
- Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) JAMA. 2002;288:2981–97. [PMID: 12479763] - PubMed
-
- Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348:383–93. [PMID: 12556541] - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560–72. [PMID: 12748199] - PubMed
-
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III) JAMA. 2001;285:2486–97. [PMID: 11368702] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials