

Early diagnosis of SARS: lessons from the Toronto SARS outbreak
- PMID: 16586072
- PMCID: PMC7087683
- DOI: 10.1007/s10096-006-0127-x
Early diagnosis of SARS: lessons from the Toronto SARS outbreak
Abstract
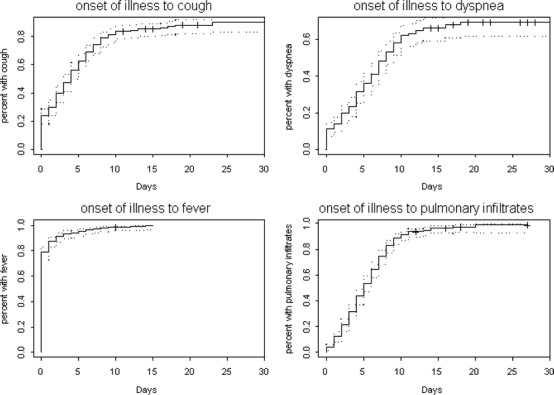
The clinical presentation of SARS is nonspecific and diagnostic tests do not provide accurate results early in the disease course. Initial diagnosis remains reliant on clinical assessment. To identify features of the clinical assessment that are useful in SARS diagnosis, the exposure status and the prevalence and timing of symptoms, signs, laboratory and radiographic findings were determined for all adult patients admitted with suspected SARS during the Toronto SARS outbreak. Findings were compared between patients with laboratory-confirmed SARS and those in whom SARS was excluded by laboratory or public health investigation. Of 364 cases, 273 (75%) had confirmed SARS, 30 (8%) were excluded, and 61 (17%) remained indeterminate. Among confirmed cases, exposure occurred in the healthcare environment (80%) or in the households of affected patients (17%); community or travel-related cases were rare (<3%). Fever occurred in 97% of patients by the time of admission. Respiratory findings including cough, dyspnea and pulmonary infiltrates evolved later and were present in only 59, 37 and 68% of patients, respectively, at admission. Direct exposure, fever on the first day of illness, and elevated temperature, pulmonary infiltrates, lymphopenia and thrombocytopenia at admission were associated with confirmed cases. Rhinorrhea, sore throat, and an elevated neutrophil count at admission were associated with excluded cases. In the absence of fever or significant exposure, SARS is unlikely. Other clinical, laboratory and radiographic findings further raise or lower the likelihood of SARS and provide a rational basis for estimating the likelihood of SARS and directing initial management.
Figures

References
-
- WHO (2004) WHO guidelines for the global surveillance of severe acute respiratory syndrome (SARS) http://www.who.int/csr/resources/publications/WHO_CDS_CSR_ARO_2004_1/en/.... Cited August 2005
-
- Lim PL, Kurup A, Gopalakrishna G, Chan KP, Wong CW, Ng LC, Se-Thoe SY, Oon L, Bai X, Stanton LW, Ruan Y, Miller LD, Vega VB, James L, Ooi PL, Kai CS, Olsen SJ, Ang B, Leo YS. Laboratory-acquired severe acute respiratory syndrome. N Engl J Med. 2004;350:1740–1745. doi: 10.1056/NEJMoa032565. - DOI - PubMed
-
- Liang G, Chen Q, Xu J, Liu Y, Lim W, Peiris JS, Anderson LJ, Ruan L, Li H, Kan B, Di B, Cheng P, Chan KH, Erdman DD, Gu S, Yan X, Liang W, Zhou D, Haynes L, Duan S, Zhang X, Zheng H, Gao Y, Tong S, Li D, Fang L, Qin P, Xu W. Laboratory diagnosis of four recent sporadic cases of community-acquired SARS, Guangdong Province, China. Emerg Infect Dis. 2004;10:1774–1781. - PMC - PubMed
-
- Poutanen SM, Low DE, Henry B, Finkelstein S, Rose D, Green K, Tellier R, Draker R, Adachi D, Ayers M, Chan AK, Skowronski DM, Salit I, Simor AE, Slutsky AS, Doyle PW, Krajden M, Petric M, Brunham RC, McGeer AJ. Identification of severe acute respiratory syndrome in Canada. N Engl J Med. 2003;348:1995–2005. doi: 10.1056/NEJMoa030634. - DOI - PubMed
-
- Booth CM, Matukas LM, Tomlinson GA, Rachlis AR, Rose DB, Dwosh HA, Walmsley SL, Mazzulli T, Avendano M, Derkach P, Ephtimios IE, Kitai I, Mederski BD, Shadowitz SB, Gold WL, Hawryluck LA, Rea E, Chenkin JS, Cescon DW, Poutanen SM, Detsky AS. Clinical features and short-term outcomes of 144 patients with SARS in the greater Toronto area. JAMA. 2003;289:2801–2809. doi: 10.1001/jama.289.21.JOC30885. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
