

Antiretroviral therapy at a district hospital in Ethiopia prevents death and tuberculosis in a cohort of HIV patients
- PMID: 16600050
- PMCID: PMC1475602
- DOI: 10.1186/1742-6405-3-10
Antiretroviral therapy at a district hospital in Ethiopia prevents death and tuberculosis in a cohort of HIV patients
Abstract
Background: Although highly active antiretroviral therapy (HAART) reduces mortality in the developed world, it remains undocumented in resource-poor settings. We assessed the effect of HAART on patient mortality and tuberculosis incidence rate under routine clinical care conditions in Ethiopia. The objective of this study was to assess the effect of HAART on patient mortality and tuberculosis incidence rate under routine clinical care conditions in a resource-limited setting in south Ethiopia. Starting in January 2003, we followed all consecutive adult HIV infected patients who visited the HIV clinic. Since August 2003, we treated patients with HAART. Only basic laboratory services were available.
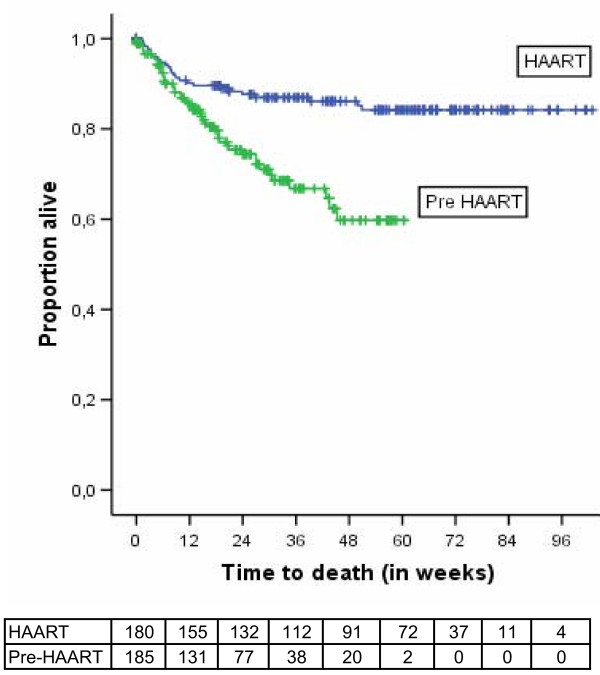
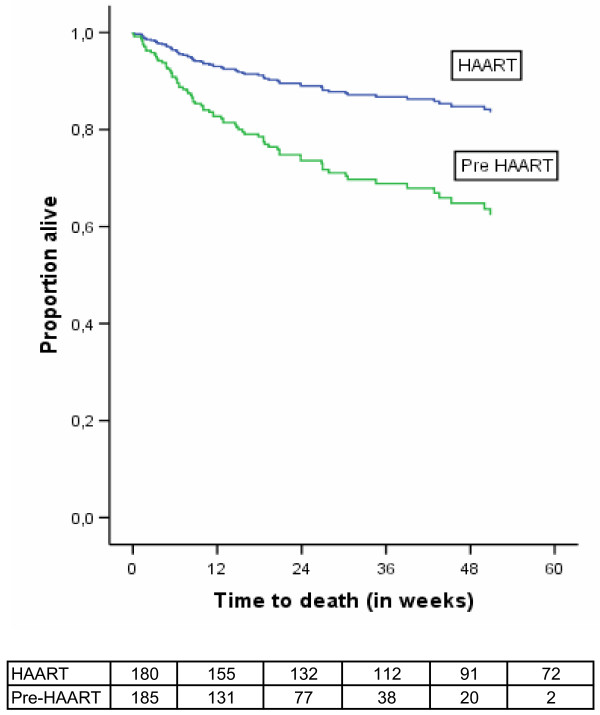
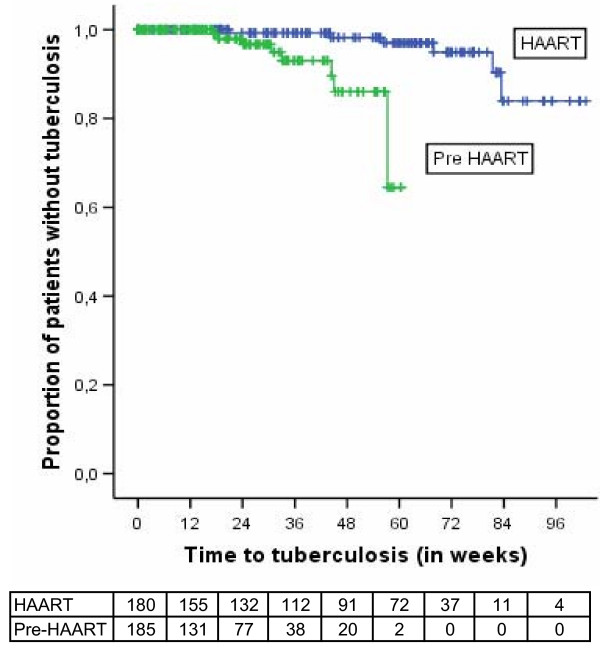
Results: We followed 185 patients in the pre-HAART cohort and 180 patients in the HAART cohort. The mortality rate was 15.4 per 100 person-years of observation (PYO) in the HAART group and tuberculosis incidence rate was 3.7 per 100 PYO. In the pre-HAART group, the mortality rate was 58.1 per 100 PYO and the tuberculosis incidence rate was 11.1 per 100 PYO. HAART resulted in a 65% decline in mortality (adjusted hazard ratio [95%CI] = 0.35 [0.19-0.63]; P < 0.001). Tuberculosis incidence rate was lower in the HAART group (adjusted hazard ratio [95%CI] = 0.11 [0.03-0.48]; P < 0.01). Most of the deaths occurred during the first three months of treatment.
Conclusion: HAART improved survival and decreased tuberculosis incidence to a level similar to that achieved in the developed countries during the early years of HAART. However, both the mortality and the tuberculosis incidence rate were much higher in terms of absolute figures in this resource-limited setting. Attention should be paid to the early weeks of treatment when mortality is high. The high tuberculosis incidence rate, when coupled with the improved survival, may lead to increased tuberculosis transmission. This highlights the need for strengthening tuberculosis prevention efforts with the scale-up of treatment programmes.
Figures
References
-
- Paul JW, Raymond M, Catherine S, Gideon R, Robert D, Debra H, Dorothy O, Peter M, Jonathan M, Badara S, Eve L. Assessment of a pilot antiretroviral therapy programme in Uganda: patients' response, survival, and drug resistance. Lancet. 2002;360:34–40. doi: 10.1016/S0140-6736(02)09330-3. - DOI - PubMed
-
- Laurent C, Ngom Gueye NF, Ndour CT, Gueye PM, Diouf M, Diakhate N, Touré Kane NC, Laniece I, Ndir A, Vergne L, Ndoye I, Mboup S, Sow PS, Delporte E. Long-Term Benefits of Highly Active Antiretroviral Therapy in Senegalese HIV-1-Infected Adults. J Acquir Immune Defic Syndr. 2005;38:14–17. doi: 10.1097/00126334-200501010-00003. - DOI - PubMed
LinkOut - more resources
Full Text Sources
