

Renal autoregulation: new perspectives regarding the protective and regulatory roles of the underlying mechanisms
- PMID: 16603656
- PMCID: PMC1578723
- DOI: 10.1152/ajpregu.00402.2005
Renal autoregulation: new perspectives regarding the protective and regulatory roles of the underlying mechanisms
Abstract
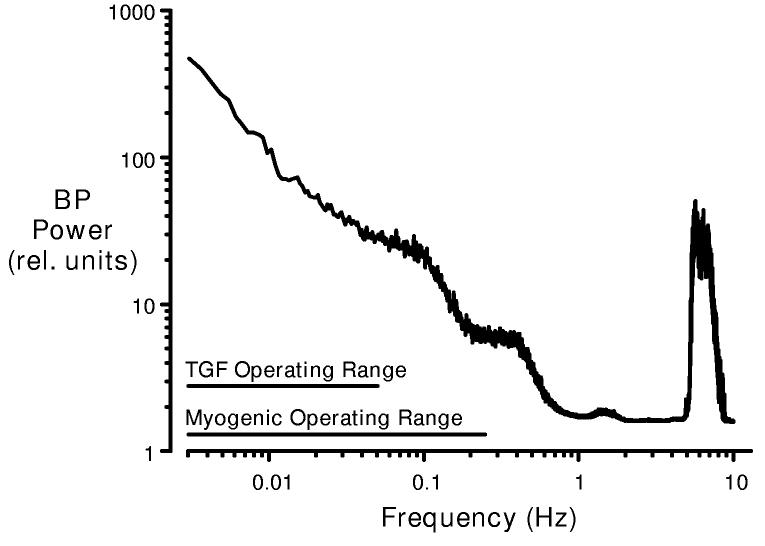
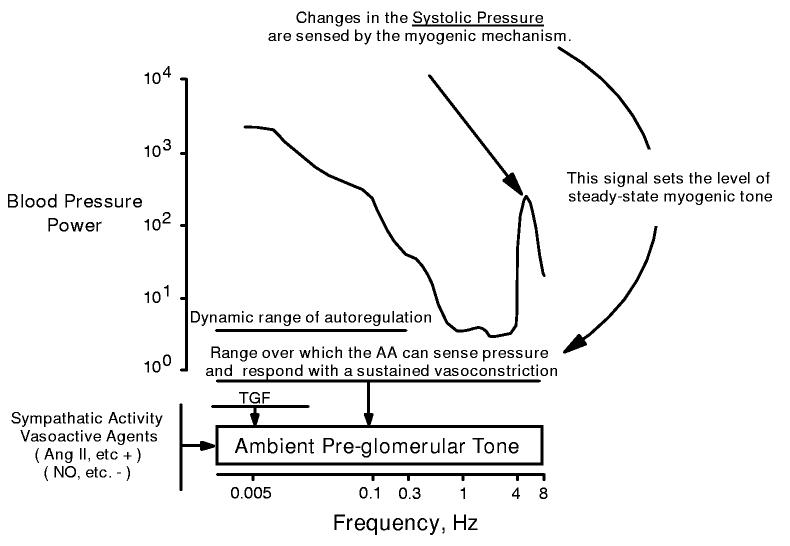
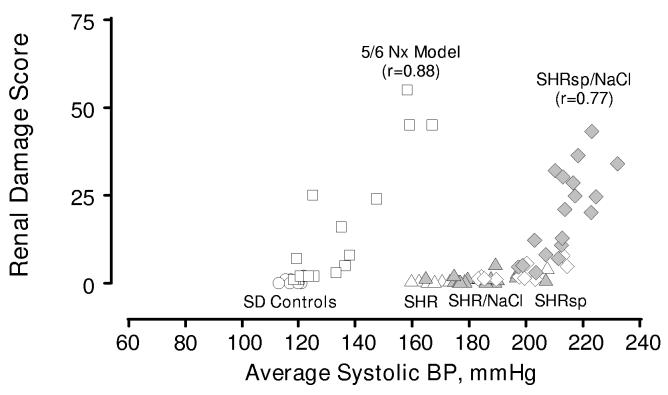
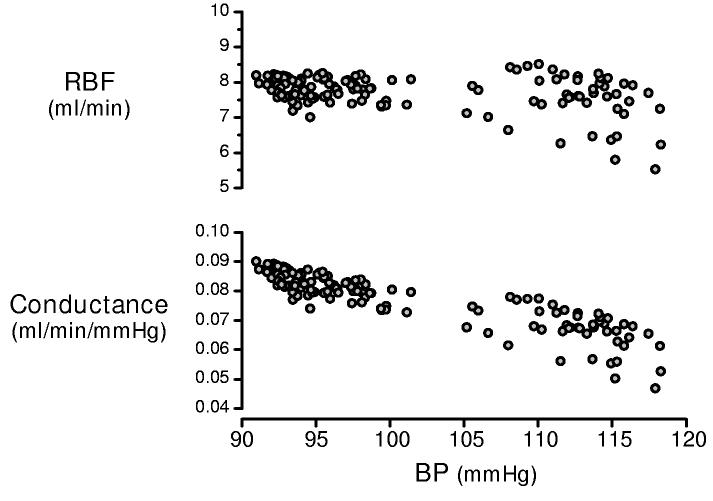
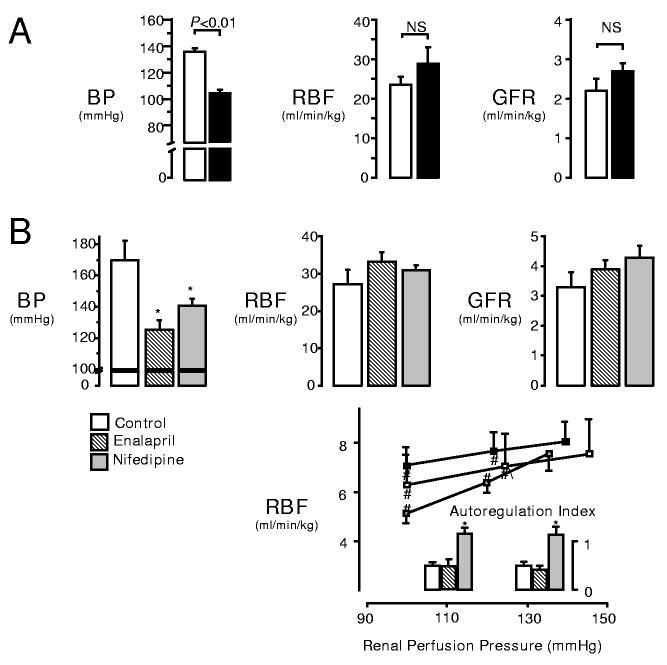
When the kidney is subjected to acute increases in blood pressure (BP), renal blood flow (RBF) and glomerular filtration rate (GFR) are observed to remain relatively constant. Two mechanisms, tubuloglomerular feedback (TGF) and the myogenic response, are thought to act in concert to achieve a precise moment-by-moment regulation of GFR and distal salt delivery. The current view is that this mechanism insulates renal excretory function from fluctuations in BP. Indeed, the concept that renal autoregulation is necessary for normal renal function and volume homeostasis has long been a cornerstone of renal physiology. This article presents a very different view, at least regarding the myogenic component of this response. We suggest that its primary purpose is to protect the kidney against the damaging effects of hypertension. The arguments advanced take into consideration the unique properties of the afferent arteriolar myogenic response that allow it to protect against the oscillating systolic pressure and the accruing evidence that when this response is impaired, the primary consequence is not a disturbed volume homeostasis but rather an increased susceptibility to hypertensive injury. It is suggested that redundant and compensatory mechanisms achieve volume regulation, despite considerable fluctuations in distal delivery, and the assumed moment-by-moment regulation of renal hemodynamics is questioned. Evidence is presented suggesting that additional mechanisms exist to maintain ambient levels of RBF and GFR within normal range, despite chronic alterations in BP and severely impaired acute responses to pressure. Finally, the implications of this new perspective on the divergent roles of the myogenic response to pressure vs. the TGF response to changes in distal delivery are considered, and it is proposed that in addition to TGF-induced vasoconstriction, vasodepressor responses to reduced distal delivery may play a critical role in modulating afferent arteriolar reactivity to integrate the regulatory and protective functions of the renal microvasculature.
Figures
References
-
- Abraham WT, Schrier RW. Body fluid volume regulation in health and disease. Adv Intern Med. 1994;39:23–47. - PubMed
-
- Abu-Amarah I, Bidani AK, Hacioglu R, Williamson GA, Griffin KA. Differential effects of salt on renal hemodynamics and potential pressure transmission in stroke-prone and stroke-resistant spontaneously hypertensive rats. Am J Physiol Renal Physiol. 2005 In press. - PubMed
-
- Arendshorst WJ. Altered reactivity of tubuloglomerular feedback. Annu Rev Physiol. 1987;49:295–317. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical