

Anterior retropharyngeal fixation C1-2 for stabilization of atlantoaxial instabilities: study of feasibility, technical description and preliminary results
- PMID: 16604355
- PMCID: PMC2438564
- DOI: 10.1007/s00586-006-0103-2
Anterior retropharyngeal fixation C1-2 for stabilization of atlantoaxial instabilities: study of feasibility, technical description and preliminary results
Abstract
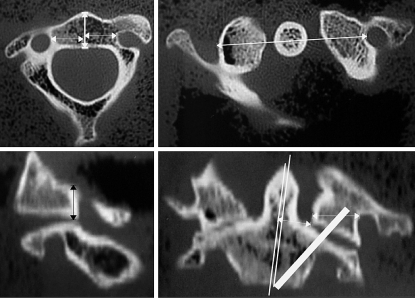
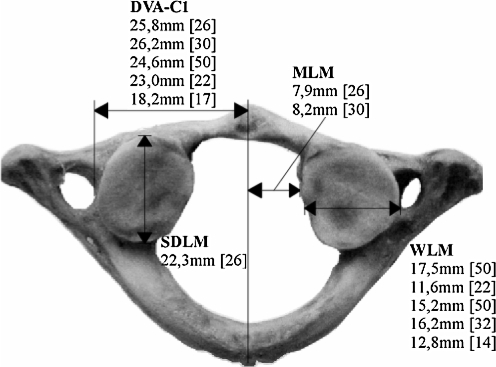
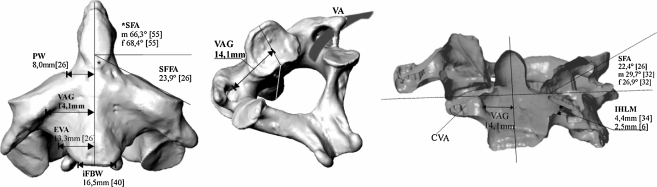
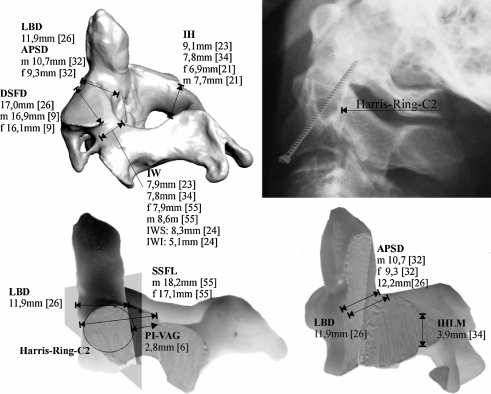
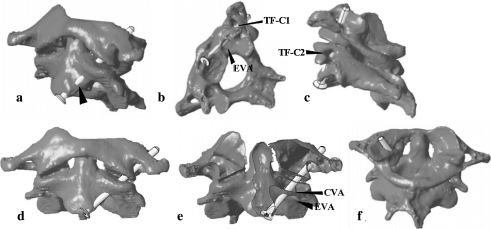
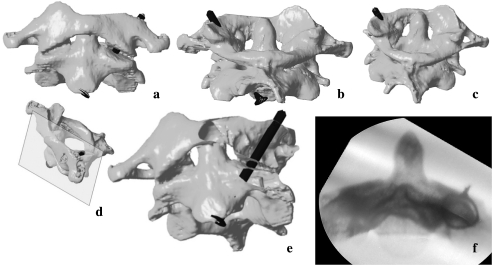
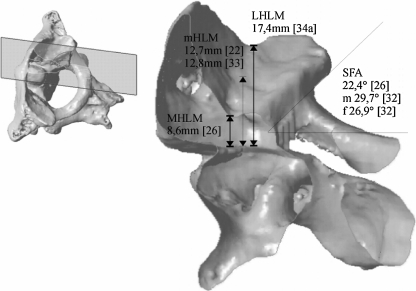
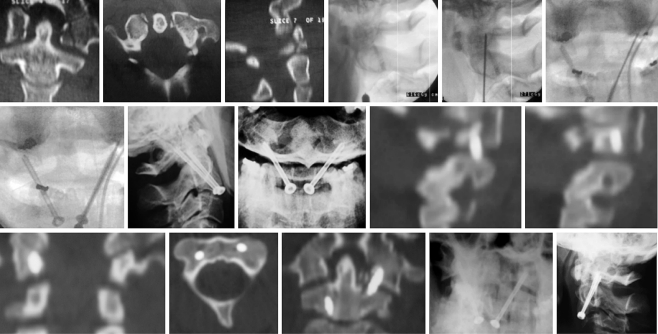
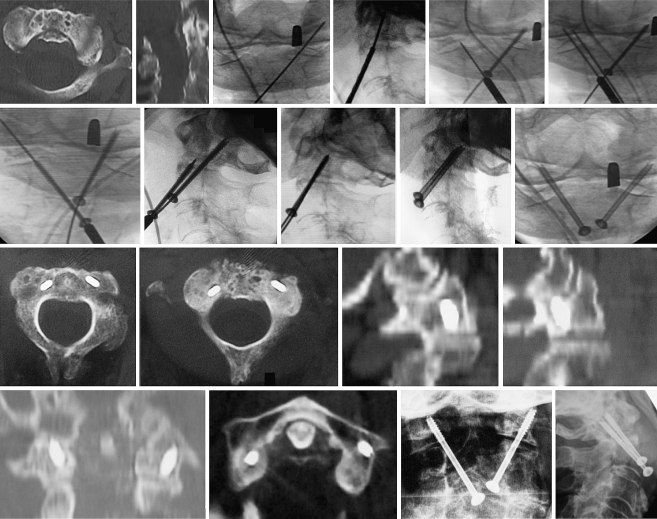
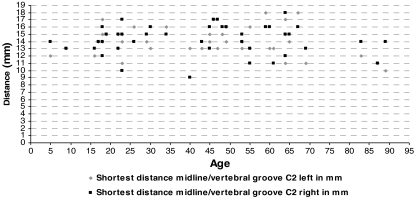
Posterior transarticular screw fixation C1-2 with the Magerl technique is a challenging procedure for stabilization of atlantoaxial instabilities. Although its high primary stability favoured it to sublaminar wire-based techniques, the close merging of the vertebral artery (VA) and its violation during screw passage inside the axis emphasizes its potential risk. Also, posterior approach to the upper cervical spine produces extensive, as well as traumatic soft-tissue stripping. In comparison, anterior transarticular screw fixation C1-2 is an atraumatic technique, but has been neglected in the literature, even though promising results are published and lectured to date. In 2004, anterior screw fixation C1-2 was introduced in our department for the treatment of atlantoaxial instabilities. As it showed convincing results, its general anatomic feasibility was worked up. The distance between mid-sagittal line of C2 and medial border of the VA groove resembles the most important anatomic landmark in anterior transarticular screw fixation C1-2. Therefore, CT based measurements on 42 healthy specimens without pathology of the cervical spine were performed. Our data are compiled in an extended collection of anatomic landmarks relevant for anterior transarticular screw fixation C1-2. Based on anatomic findings, the technique and its feasibility in daily clinical work is depicted and discussed on our preliminary results in seven patients.
Figures

References
-
- Apostolides PJ, Theodore N, Karahalios DG, Sonntag VK (1997) Triple anterior screw fixation of an acute combination atlas-axis fracture. J Neurosurg 87:96–99 - PubMed
-
- Barbour JR (1971) Screw fixation in fractures of the odontoid process. S Aust Clinics 5:20
-
- Bremerich FH, Dvorak J, Mannion AF, Grob D (2003) Long-term results after posterior transarticular C1–C2 fusion lecture. CSRS-E, Barcelona, Spain
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
