

The effect of alpha+-thalassaemia on the incidence of malaria and other diseases in children living on the coast of Kenya
- PMID: 16605300
- PMCID: PMC1435778
- DOI: 10.1371/journal.pmed.0030158
The effect of alpha+-thalassaemia on the incidence of malaria and other diseases in children living on the coast of Kenya
Abstract
Background: The alpha-thalassaemias are the commonest genetic disorders of humans. It is generally believed that this high frequency reflects selection through a survival advantage against death from malaria; nevertheless, the epidemiological description of the relationships between alpha-thalassaemia, malaria, and other common causes of child mortality remains incomplete.
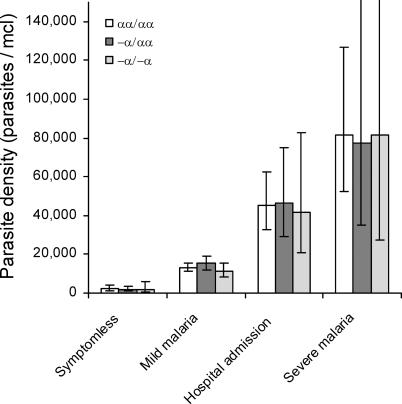
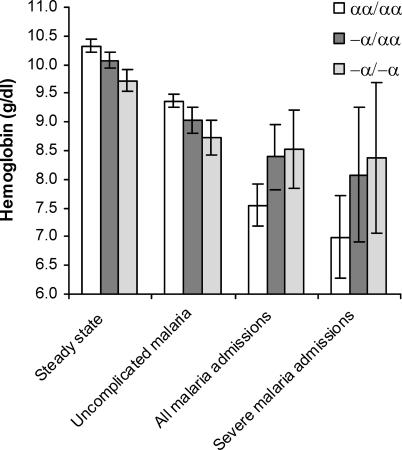
Methods and findings: We studied the alpha+-thalassaemia-specific incidence of malaria and other common childhood diseases in two cohorts of children living on the coast of Kenya. We found no associations between alpha+-thalassaemia and the prevalence of symptomless Plasmodium falciparum parasitaemia, the incidence of uncomplicated P. falciparum disease, or parasite densities during mild or severe malaria episodes. However, we found significant negative associations between alpha+-thalassaemia and the incidence rates of severe malaria and severe anaemia (haemoglobin concentration < 50 g/l). The strongest associations were for severe malaria anaemia (> 10,000 P. falciparum parasites/mul) and severe nonmalaria anaemia; the incidence rate ratios and 95% confidence intervals (CIs) for alpha+-thalassaemia heterozygotes and homozygotes combined compared to normal children were, for severe malaria anaemia, 0.33 (95% CI, 0.15,0.73; p = 0.006), and for severe nonmalaria anaemia, 0.26 (95% CI, 0.09,0.77; p = 0.015).
Conclusions: Our observations suggest, first that selection for alpha+-thalassaemia might be mediated by a specific effect against severe anaemia, an observation that may lead to fresh insights into the aetiology of this important condition. Second, although alpha+-thalassaemia is strongly protective against severe and fatal malaria, its effects are not detectable at the level of any other malaria outcome; this result provides a cautionary example for studies aimed at testing malaria interventions or identifying new malaria-protective genes.
Conflict of interest statement
Figures
Comment in
-
Does alpha+-thalassaemia protect against malaria?PLoS Med. 2006 May;3(5):e235. doi: 10.1371/journal.pmed.0030235. Epub 2006 May 9. PLoS Med. 2006. PMID: 16646635 Free PMC article.
References
-
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet. 1997;349:1436–1442. - PubMed
-
- Snow RW, Craig MH, Newton CRJC, Steketee RW. The public health burden of P. falciparum malaria in Africa: Deriving the numbers . Bethesda: Fogerty International Center, National Institutes of Health; 2003.
-
- Flint J, Harding RM, Boyce AJ, Clegg JB. The population genetics of the haemoglobinopathies. Baillieres Clin Haematol. 1998;11:1–51. - PubMed
-
- Weatherall DJ, Clegg JB. The thalassaemia syndromes. 4th ed. Oxford: Blackwell Science; 2001. 846 pp.
