

Minimally invasive 'step-up approach' versus maximal necrosectomy in patients with acute necrotising pancreatitis (PANTER trial): design and rationale of a randomised controlled multicenter trial [ISRCTN13975868]
- PMID: 16606471
- PMCID: PMC1508161
- DOI: 10.1186/1471-2482-6-6
Minimally invasive 'step-up approach' versus maximal necrosectomy in patients with acute necrotising pancreatitis (PANTER trial): design and rationale of a randomised controlled multicenter trial [ISRCTN13975868]
Abstract
Background: The initial treatment of acute necrotizing pancreatitis is conservative. Intervention is indicated in patients with (suspected) infected necrotizing pancreatitis. In the Netherlands, the standard intervention is necrosectomy by laparotomy followed by continuous postoperative lavage (CPL). In recent years several minimally invasive strategies have been introduced. So far, these strategies have never been compared in a randomised controlled trial. The PANTER study (PAncreatitis, Necrosectomy versus sTEp up appRoach) was conceived to yield the evidence needed for a considered policy decision.
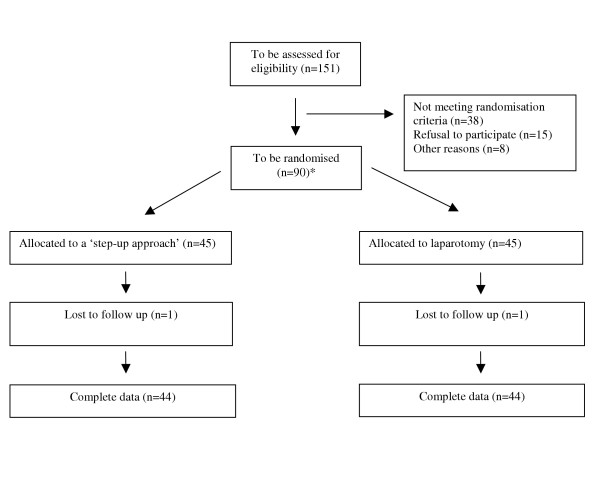
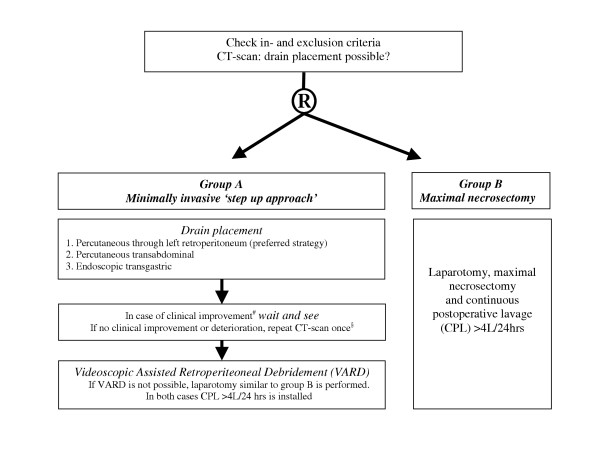
Methods/design: 88 patients with (suspected) infected necrotizing pancreatitis will be randomly allocated to either group A) minimally invasive 'step-up approach' starting with drainage followed, if necessary, by videoscopic assisted retroperitoneal debridement (VARD) or group B) maximal necrosectomy by laparotomy. Both procedures are followed by CPL. Patients will be recruited from 20 hospitals, including all Dutch university medical centres, over a 3-year period. The primary endpoint is the proportion of patients suffering from postoperative major morbidity and mortality. Secondary endpoints are complications, new onset sepsis, length of hospital and intensive care stay, quality of life and total (direct and indirect) costs. To demonstrate that the 'step-up approach' can reduce the major morbidity and mortality rate from 45 to 16%, with 80% power at 5% alpha, a total sample size of 88 patients was calculated.
Discussion: The PANTER-study is a randomised controlled trial that will provide evidence on the merits of a minimally invasive 'step-up approach' in patients with (suspected) infected necrotizing pancreatitis.
Figures
References
-
- Bradley EL., III A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg. 1993;128:586–590. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
