

Heterozygous familial hypercholesterolemia: an underrecognized cause of early cardiovascular disease
- PMID: 16606962
- PMCID: PMC1421462
- DOI: 10.1503/cmaj.051313
Heterozygous familial hypercholesterolemia: an underrecognized cause of early cardiovascular disease
Abstract
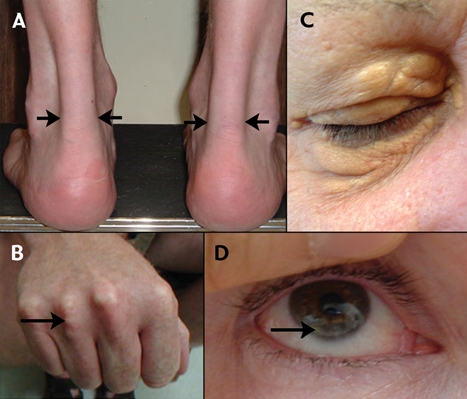
Heterozygous familial hypercholesterolemia (HeFH) is a monogenic disorder that affects about 1 in 500 people, with a higher prevalence in certain subpopulations such as people of Quebecois, Christian Lebanese and Dutch South Afrikaner extraction. HeFH is characterized by cholesterol deposits affecting the corneas, eyelids and extensor tendons; elevated plasma concentrations of low-density lipoprotein (LDL) cholesterol; and accelerated vascular disease, especially coronary artery disease (CAD). Although HeFH is genetically heterogeneous, it is most often caused by heterozygous mutations in the LDLR gene encoding the LDL receptor. We describe a man who was diagnosed with HeFH after he had a myocardial infarction at 33 years of age. By DNA sequence analysis, he was found to have a heterozygous splicing mutation in his LDLR gene. This discovery expanded the growing mutational spectrum in patients with HeFH in Ontario. Given that HeFH is a treatable cause of early vascular disease, it is important that this condition be recognized, diagnosed and treated in affected patients; but as yet, there is no consensus on the best approach. Diagnostic criteria based on family history and clinical presentation have been proposed for patients with suspected HeFH. Biochemical or molecular screening might be considered to detect new cases of HeFH in populations with a relatively high HeFH prevalence and a relatively small number of possible causative mutations. So far, however, the most cost-effective and efficient systematic strategy to detect previously undiagnosed cases of HeFH is still cascade testing: clinical and biochemical screening of close relatives of the proband patient diagnosed with HeFH. Pharmacologic treatment of HeFH is cost-effective.
Figures


References
-
- Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis. Science 1986;232:34-47. - PubMed
-
- Word Health Organization—Human Genetics (editors). DoNDP, familial hypercholesterolaemia: report of a second WHO Consultation. Geneva: WHO; 1999.
-
- Kuch B, Bolte HD, Hoermann A, et al. What is the real hospital mortality from acute myocardial infarction? Eur Heart J 2002;23:714-20. - PubMed
-
- Rosamond WD, Chamblesss LE, Folsom AR, et al. Trends in the incidence of myocardial infarction and in mortality due to coronary heart disease, 1987 to 1994. N Engl J Med 1998;339:861-7. - PubMed
-
- Takada D, Emi M, Ezura Y, et al. Interaction between the LDL-receptor gene bearing a novel mutation and a variant in the apolipoprotein A-II promoter: molecular study in a 1135-member familial hypercholesterolemia kindred. J Hum Genet 2002; 47:656-64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous