

Surgical anatomy of the innervation of pylorus in human and Suncus murinus, in relation to surgical technique for pylorus-preserving pancreaticoduodenectomy
- PMID: 16610023
- PMCID: PMC4087648
- DOI: 10.3748/wjg.v12.i14.2209
Surgical anatomy of the innervation of pylorus in human and Suncus murinus, in relation to surgical technique for pylorus-preserving pancreaticoduodenectomy
Abstract
Aim: To clarify the innervation of the antro-pyloric region in humans from a clinico-anatomical perspective.
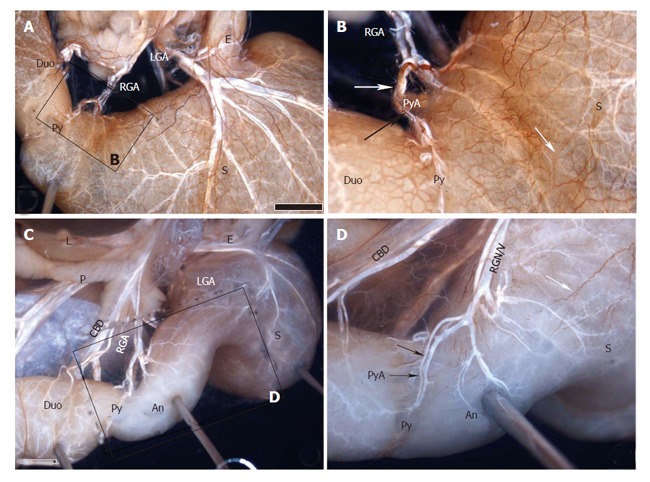
Methods: The stomach, duodenum and surrounding structures were dissected in 10 cadavers, and immersed in a 10mg/L solution of alizarin red S in ethanol to stain the peripheral nerves. The distribution details were studied to confirm innervations in the above areas using a binocular microscope. Similarly, innervations in 10 Suncus murinus were examined using the method of whole-mount immunohistochemistry.
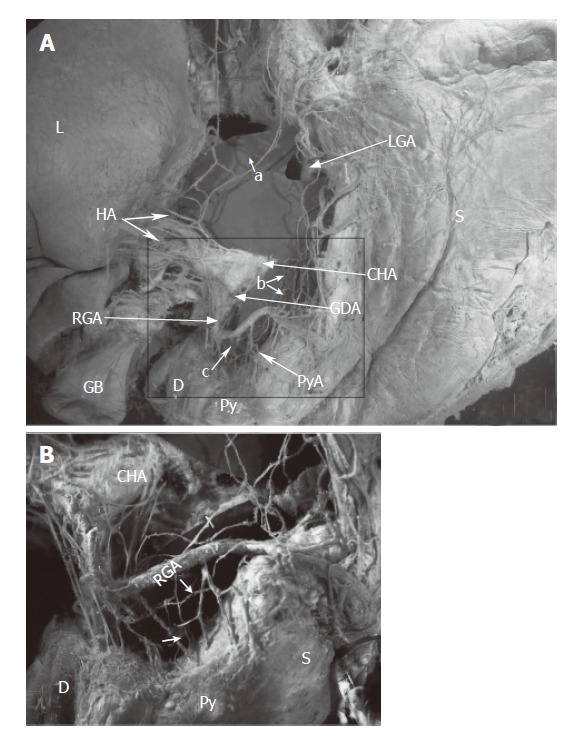
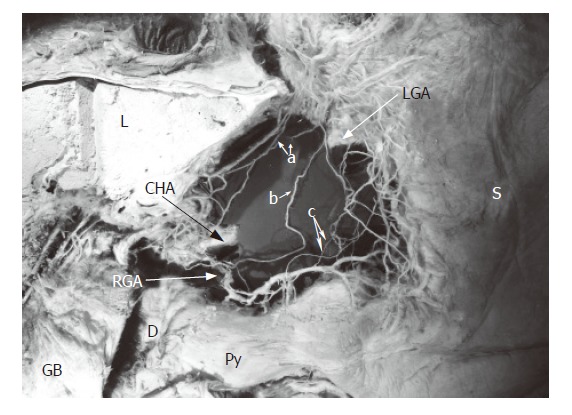
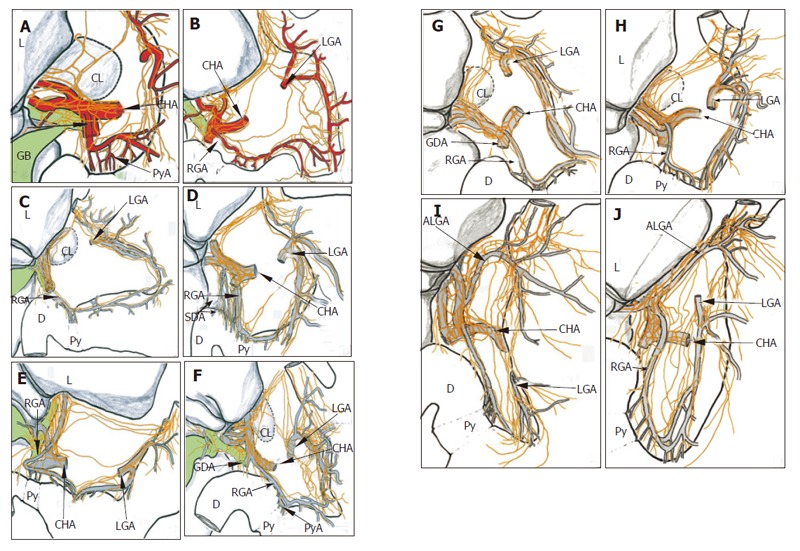
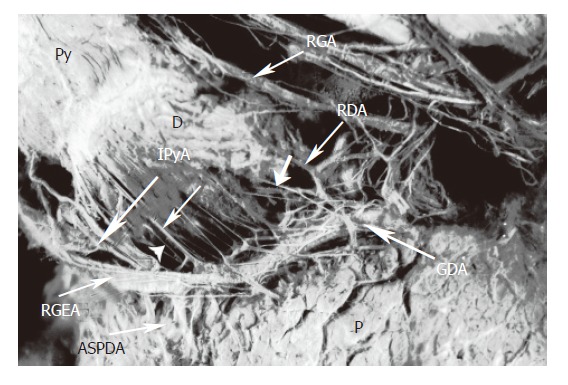
Results: The innervation of the pyloric region in humans involved three routes: One arose from the anterior hepatic plexus via the route of the suprapyloric/supraduodenal branch of the right gastric artery; the second arose from the anterior and posterior gastric divisions, and the third originated from the posterior-lower region of the pyloric region, which passed via the infrapyloric artery or retroduodenal branches and was related to the gastroduodenal artery and right gastroepiploic artery. For Suncus murinus, results similar to those in humans were observed.
Conclusion: There are three routes of innervation of the pyloric region in humans, wherein the route of the right gastric artery is most important for preserving pyloric region innervation. Function will be preserved by more than 80% by preserving the artery in pylorus-preserving pancreaticoduodenectomy (PPPD). However, the route of the infrapyloric artery should not be disregarded. This route is related to several arteries (the right gastroepiploic and gastroduodenal arteries), and the preserving of these arteries is advantageous for preserving pyloric innervation in PPPD. Concurrently, the nerves of Latarjet also play an important role in maintaining innervation of the antro-pyloric region in PPPD. This is why pyloric function is not damaged in some patients when the right gastric artery is dissected or damaged in PPPD.
Figures
Similar articles
-
Surgical anatomy of innervation of the gallbladder in humans and Suncus murinus with special reference to morphological understanding of gallstone formation after gastrectomy.World J Gastroenterol. 2007 Apr 14;13(14):2066-71. doi: 10.3748/wjg.v13.i14.2066. World J Gastroenterol. 2007. PMID: 17465449 Free PMC article.
-
Surgical anatomy of the innervation of the major duodenal papilla in human and Suncus murinus, from the perspective of preserving innervation in organ-saving procedures.Pancreas. 2005 Apr;30(3):211-7. doi: 10.1097/01.mpa.0000158027.38548.34. Pancreas. 2005. PMID: 15782096
-
The infrapyloric artery and cephalic pancreatoduodenectomy with pylorus preservation: preliminary study.Surg Radiol Anat. 1994;16(2):165-72. doi: 10.1007/BF01627590. Surg Radiol Anat. 1994. PMID: 7940080
-
Pancreaticoduodenectomy versus pylorus-preserving pancreaticoduodenectomy: the clinical impact of a new surgical procedure; pylorus-resecting pancreaticoduodenectomy.J Hepatobiliary Pancreat Sci. 2011 Nov;18(6):755-61. doi: 10.1007/s00534-011-0427-0. J Hepatobiliary Pancreat Sci. 2011. PMID: 21861144 Review.
-
Meta-analysis of subtotal stomach-preserving pancreaticoduodenectomy vs pylorus preserving pancreaticoduodenectomy.World J Gastroenterol. 2015 May 28;21(20):6361-73. doi: 10.3748/wjg.v21.i20.6361. World J Gastroenterol. 2015. PMID: 26034372 Free PMC article. Review.
Cited by
-
Surgical anatomy of innervation of the gallbladder in humans and Suncus murinus with special reference to morphological understanding of gallstone formation after gastrectomy.World J Gastroenterol. 2007 Apr 14;13(14):2066-71. doi: 10.3748/wjg.v13.i14.2066. World J Gastroenterol. 2007. PMID: 17465449 Free PMC article.
-
Gut microbiota of Suncus murinus, a naturally obesity-resistant animal, improves the ecological diversity of the gut microbiota in high-fat-diet-induced obese mice.PLoS One. 2023 Nov 22;18(11):e0293213. doi: 10.1371/journal.pone.0293213. eCollection 2023. PLoS One. 2023. PMID: 37992054 Free PMC article.
-
Using a Whole-mount Immunohistochemical Method to Study the Innervation of the Biliary Tract in Suncus murinus.J Vis Exp. 2017 Jun 15;(124):55483. doi: 10.3791/55483. J Vis Exp. 2017. PMID: 28654062 Free PMC article.
-
Excellent oncological outcomes besides short-term safety of laparoscopic and endoscopic cooperative surgery for gastric gastrointestinal stromal tumor.Endosc Int Open. 2022 Sep 14;10(9):E1254-E1260. doi: 10.1055/a-1895-9507. eCollection 2022 Sep. Endosc Int Open. 2022. PMID: 36118650 Free PMC article.
-
Function-preserving surgery for gastric cancer.Int J Clin Oncol. 2006 Oct;11(5):357-66. doi: 10.1007/s10147-006-0613-2. Int J Clin Oncol. 2006. PMID: 17058133 Review.
References
-
- Traverso LW, Longmire WP. Preservation of the pylorus in pancreaticoduodenectomy. Surg Gynecol Obstet. 1978;146:959–962. - PubMed
-
- Ueno T, Tanaka A, Hamanaka Y, Tsurumi M, Suzuki T. A proposal mechanism of early delayed gastric emptying after pylorus preserving pancreatoduodenectomy. Hepatogastroenterology. 1995;42:269–274. - PubMed
-
- Yamaguchi K, Kishinaka M, Nagai E, Nakano K, Ohtsuka T, Chijiwa K, Tanaka M. Pancreatoduodenectomy for pancreatic head carcinoma with or without pylorus preservation. Hepatogastroenterology. 2001;48:1479–1485. - PubMed
-
- Sugiyama M, Abe N, Ueki H, Masaki T, Mori T, Atomi Y. A new reconstruction method for preventing delayed gastric emptying after pylorus-preserving pancreatoduodenectomy. Am J Surg. 2004;187:743–746. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
