

Combinations of the presence or absence of cerebral microbleeds and advanced white matter hyperintensity as predictors of subsequent stroke types
- PMID: 16611773
- PMCID: PMC8133980
Combinations of the presence or absence of cerebral microbleeds and advanced white matter hyperintensity as predictors of subsequent stroke types
Abstract
Background and purpose: Previous studies have shown microbleeds to be a risk factor for intracerebral hemorrhage and white matter hyperintensity (WMH) to be a risk factor for ischemic stroke. This study was performed to determine whether combinations of the presence or absence of microbleeds and advanced WMH are risk factors for subsequent recurrent stroke types.
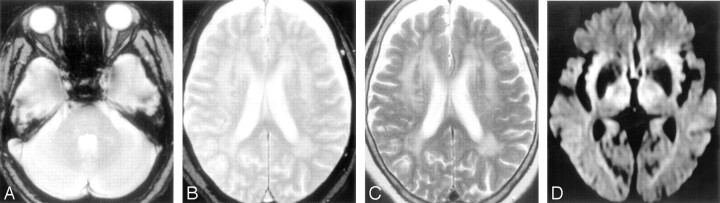
Methods: In 266 patients with stroke, microbleeds on T2*-weighted MR images were counted, and WMH on T2-weighted images was graded. Patients were divided into 4 groups by the combinations of the presence or absence of microbleeds and advanced WMH and were followed up for stroke recurrence.
Results: During a mean follow-up period of 564.8 +/- 220.5 days, 26 patients developed recurrent strokes, including 10 intracerebral hemorrhages and 16 ischemic strokes. Patients with microbleeds without advanced WMH (n = 42) developed only intracerebral hemorrhages (n = 8), and the recurrence rate of intracerebral hemorrhage in those patients estimated by the Kaplan-Meier method was the highest in the 4 groups (14.3% in 1 year and 21.2% in 2 years). In contrast, patients with advanced WMH without microbleeds (n = 39) developed only ischemic strokes (n = 6), and the estimated recurrent rate of ischemic stroke in those patients was the highest in the 4 groups (10.5% in 1 year and 17.4% in 2 years). Cox proportional hazards regression analysis revealed that microbleeds were associated with intracerebral hemorrhage (hazard ratio [HR], 85.626; 95% confidence interval [CI], 6.344-1155.649) and that advanced WMH was negatively associated with intracerebral hemorrhage (HR, 0.016; 95% CI, 0.001-0.258). Advanced WMH was associated with ischemic stroke (HR, 10.659; 95% CI, 2.601-43.678).
Conclusion: It appears that patients at high risk of subsequent intracerebral hemorrhage or ischemic stroke can be identified by combinations of the presence or absence of microbleeds and advanced WMH.
Figures

Comment in
-
Do poststroke MRI findings predict the type of a subsequent stroke?Nat Clin Pract Neurol. 2007 Jan;3(1):20-1. doi: 10.1038/ncpneuro0377. Nat Clin Pract Neurol. 2007. PMID: 17205070 No abstract available.
References
-
- Tanaka A, Ueno Y, Nakayama Y, et al. Small chronic hemorrhages and ischemic lesions in association with spontaneous intracerebral hematomas. Stroke 1999;30:1637–42 - PubMed
-
- Kwa VIH, Franke CL, Verbeeten B Jr, et al. Silent intracerebral microhemorrhages in patients with ischemic stroke. Ann Neurol 1998;44:372–77 - PubMed
-
- Roob G, Lechner A, Schmidt R, et al. Frequency and location of microbleeds in patients with primary intracerebral hemorrhage. Stroke 2000;31:2665–69 - PubMed
-
- Kato H, Izumiyama M, Izumiyama K, et al. Silent cerebral microbleeds on T2*-weighted MRI: correlation with stroke subtype, stroke recurrence, and leukoaraiosis. Stroke 2002;33:1536–40 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical