

Do cerebral blood volume and contrast transfer coefficient predict prognosis in human glioma?
- PMID: 16611778
- PMCID: PMC8133992
Do cerebral blood volume and contrast transfer coefficient predict prognosis in human glioma?
Abstract
Introduction: Noninvasive measurements of cerebral blood volume (CBV) and contrast transfer coefficient (K(trans)) have potential benefits in the diagnosis and therapeutic management of adult glioma. This study examines the relationship between CBV, K(trans), and overall survival.
Methods and materials: Twenty-seven adult patients with glioma underwent T1-weighted dynamic contrast-enhanced MR imaging, and parametric maps of CBV and K(trans) were calculated. The relationship of histologic grade, CBV, K(trans), age, sex, surgical resection, and use of adjuvant therapy to survival were analyzed by using the logrank method and Cox regression analysis. The Kaplan-Meier method for displaying survival curves was used. The relationship of factors such as comorbidity, elevated intracranial pressure, size of nonenhancing tumor, and peritumoral edema were not considered.
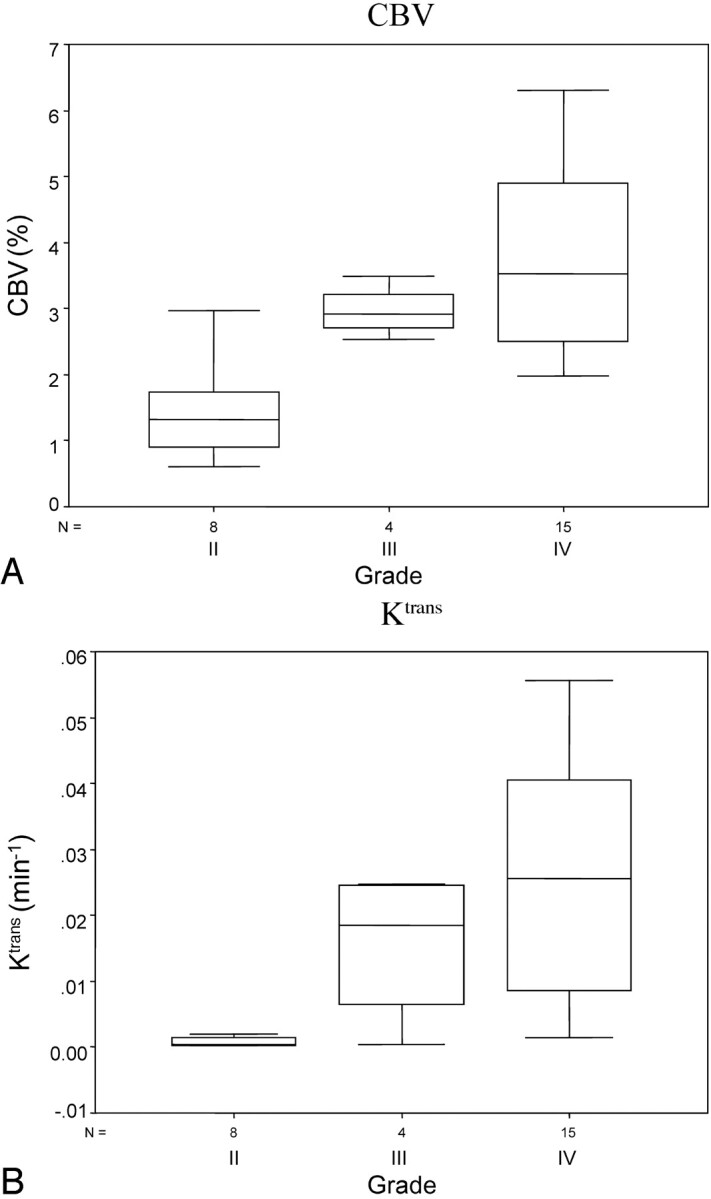
Results: Both CBV (P < .01) and K(trans) (P < .01) show a significant relationship to histologic grade. CBV (P = .004), K(trans) (P = .008), and histologic grade (P < .001) all demonstrate a significant association with patient survival when analyzed individually. Cox regression analysis identified only histologic grade (P < .01) and K(trans) (P < .05) as independent significant prognostic indicators. Examination of survival data from high-grade (III and IV) tumors demonstrated a linear relationship between K(trans) and patient survival (P < .01).
Conclusion: This study suggests a direct relationship between K(trans) and length of survival in high-grade gliomas, which could be of clinical importance. CBV relates directly to histologic grade but provides no independent prognostic information over and above that provided by grade. Further large prospective studies should be planned to test whether this observation holds true.
Figures




References
-
- Wyllie AD. Growth and neoplasia. In: MacSween N, Whaley K. Muir’s textbook of pathology. 13th ed. London: Edward Arnold;1992;355–410
-
- Plate KH, Breier G, Weich HA, et al., Vascular endothelial growth factor is a potential tumour angiogenesis factor in human gliomas in vivo. Nature 1992;359:845–48 - PubMed
-
- Dvorak HF, Brown LF, Detmar M, et al. Vascular permeability factor/vascular endothelial growth factor: an important mediator of angiogenesis in malignancy and inflammation. Int Arch Allergy Immunol 1995;107:233–35 - PubMed
-
- Chaudhry IH, O’Donovan DG, Brenchley PEC, et al. Vascular endothelial growth factor expression correlates with tumour grade and vascularity in gliomas. Histopathology 2001;39:409–15 - PubMed
-
- Warmuth C, Gunther M, Zimmer C. Quantification of blood flow in brain tumors: comparison of arterial spin labeling and dynamic susceptibility-weighted contrast-enhanced MR imaging. Radiology 2003;228:523–32 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical