

Multivariable risk prediction can greatly enhance the statistical power of clinical trial subgroup analysis
- PMID: 16613605
- PMCID: PMC1523355
- DOI: 10.1186/1471-2288-6-18
Multivariable risk prediction can greatly enhance the statistical power of clinical trial subgroup analysis
Abstract
Background: When subgroup analyses of a positive clinical trial are unrevealing, such findings are commonly used to argue that the treatment's benefits apply to the entire study population; however, such analyses are often limited by poor statistical power. Multivariable risk-stratified analysis has been proposed as an important advance in investigating heterogeneity in treatment benefits, yet no one has conducted a systematic statistical examination of circumstances influencing the relative merits of this approach vs. conventional subgroup analysis.
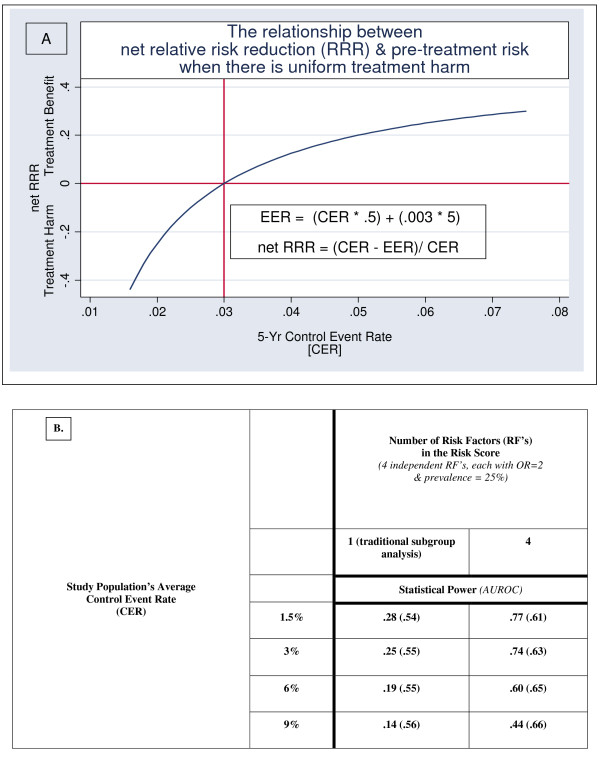
Methods: Using simulated clinical trials in which the probability of outcomes in individual patients was stochastically determined by the presence of risk factors and the effects of treatment, we examined the relative merits of a conventional vs. a "risk-stratified" subgroup analysis under a variety of circumstances in which there is a small amount of uniformly distributed treatment-related harm. The statistical power to detect treatment-effect heterogeneity was calculated for risk-stratified and conventional subgroup analysis while varying: 1) the number, prevalence and odds ratios of individual risk factors for risk in the absence of treatment, 2) the predictiveness of the multivariable risk model (including the accuracy of its weights), 3) the degree of treatment-related harm, and 5) the average untreated risk of the study population.
Results: Conventional subgroup analysis (in which single patient attributes are evaluated "one-at-a-time") had at best moderate statistical power (30% to 45%) to detect variation in a treatment's net relative risk reduction resulting from treatment-related harm, even under optimal circumstances (overall statistical power of the study was good and treatment-effect heterogeneity was evaluated across a major risk factor [OR = 3]). In some instances a multi-variable risk-stratified approach also had low to moderate statistical power (especially when the multivariable risk prediction tool had low discrimination). However, a multivariable risk-stratified approach can have excellent statistical power to detect heterogeneity in net treatment benefit under a wide variety of circumstances, instances under which conventional subgroup analysis has poor statistical power.
Conclusion: These results suggest that under many likely scenarios, a multivariable risk-stratified approach will have substantially greater statistical power than conventional subgroup analysis for detecting heterogeneity in treatment benefits and safety related to previously unidentified treatment-related harm. Subgroup analyses must always be well-justified and interpreted with care, and conventional subgroup analyses can be useful under some circumstances; however, clinical trial reporting should include a multivariable risk-stratified analysis when an adequate externally-developed risk prediction tool is available.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
