

Relative corticosteroid insensitivity of peripheral blood mononuclear cells in severe asthma
- PMID: 16614347
- PMCID: PMC2662905
- DOI: 10.1164/rccm.200512-1930OC
Relative corticosteroid insensitivity of peripheral blood mononuclear cells in severe asthma
Abstract
Rationale and objectives: Patients with severe asthma have a poor therapeutic response to corticosteroid therapy, and corticosteroid responsiveness cannot be easily measured in these patients. We hypothesized that this poor response is associated with a reduced effect of corticosteroids to inhibit cytokine release from activated peripheral blood mononuclear cells (PBMCs).
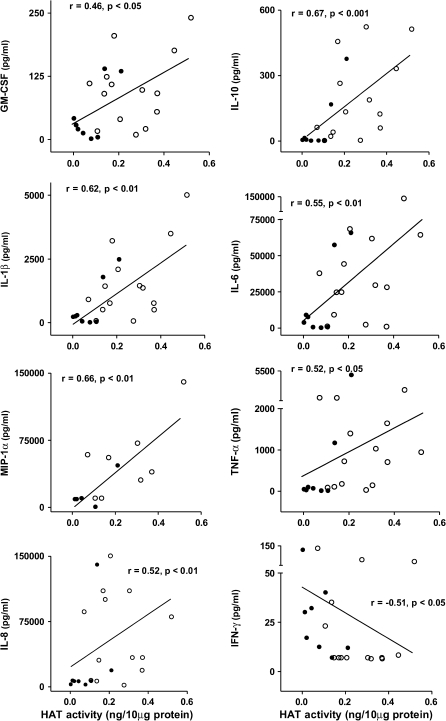
Methods: Patients with severe asthma were defined by American Thoracic Society criteria. We compared the suppression of LPS-induced cytokine release (monocyte chemotactic protein-1 [MCP-1], macrophage inflammatory protein [MIP] 1alpha, RANTES, tumor necrosis factor alpha, interleukin 1beta (IL-1beta), IL-8, IFN-gamma, IL-6, IL-10, and granulocyte-macrophage colony-stimulating factor [GM-CSF]) by dexamethasone from PBMCs of patients with severe asthma (n = 16), patients with nonsevere asthma (n = 19), and normal volunteers (n = 10).
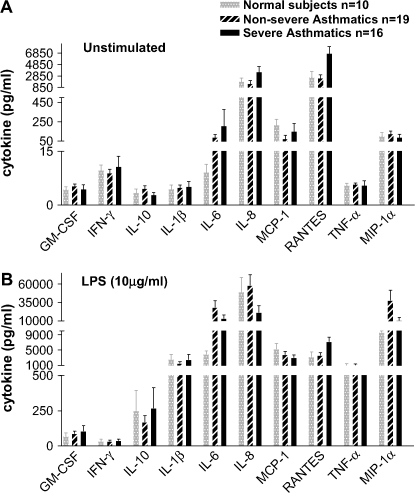
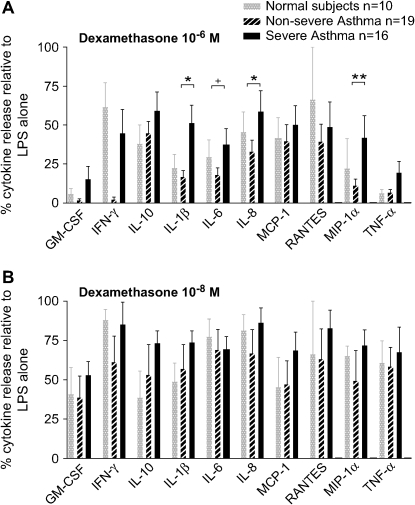
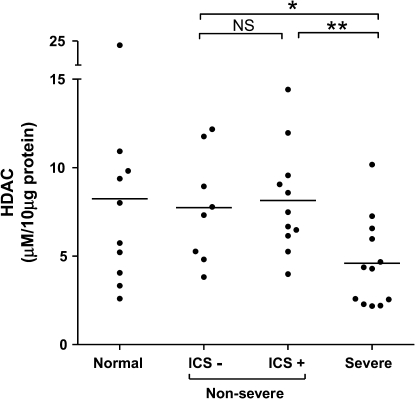
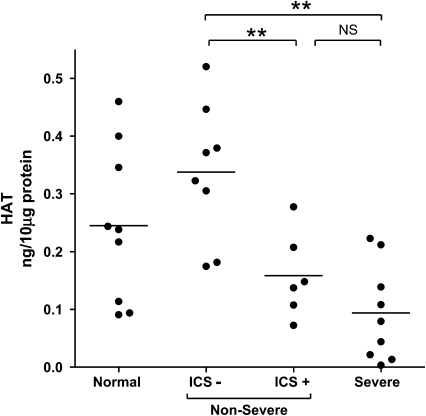
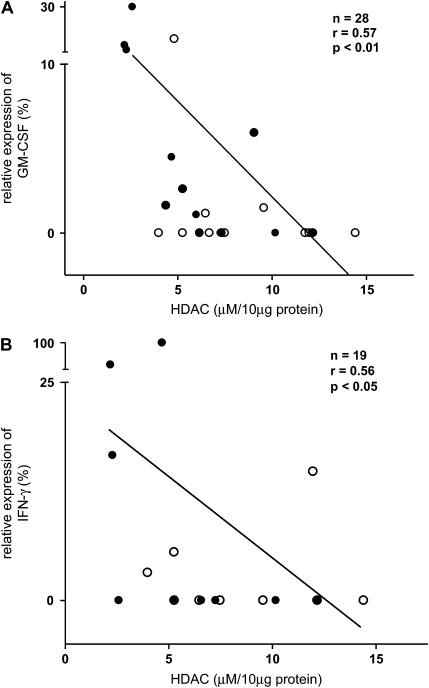
Results: There was no difference in baseline spontaneous or stimulated release of these cytokines among groups. LPS-induced release of 10 cytokines was less suppressed by dexamethasone (10(-6) M) in patients with severe asthma compared with patients with nonsevere asthma, with statistical significance achieved for IL-1beta (p < 0.03), IL-8 (p < 0.03), and MIP-1alpha (p < 0.003), and borderline significance for IL-6 (p = 0.054). There was less difference between the two groups for dexamethasone at 10(-8) M. Nuclear histone deacetylase (HDAC) and histone acetyltransferase activities were reduced in patients with severe asthma compared with patients with nonsevere asthma (p < 0.01). HDAC activity reduction correlated directly to the degree of steroid insensitivity of GM-CSF (r = 0.57, p < 0.01) and IFN-gamma (r = 0.56, p < 0.05) release. Reduction in histone acetyltransferase activity related to corticosteroid use rather than asthma severity.
Conclusions: Patients with severe asthma have diminished corticosteroid sensitivity of PBMCs when compared with patients with nonsevere asthma, associated with a reduction in HDAC activity that parallels the impaired corticosteroid sensitivity.
Figures
References
-
- American Thoracic Society. Proceedings of the ATS workshop on refractory asthma: current understanding, recommendations, and unanswered questions. Am J Respir Crit Care Med 2000;162:2341–2351. - PubMed
-
- Chung KF, Godard P, Adelroth E, Ayres J, Barnes N, Barnes P, Bel E, Burney P, Chanez P, Connett G, et al. Difficult/therapy-resistant asthma: the need for an integrated approach to define clinical phenotypes, evaluate risk factors, understand pathophysiology and find novel therapies. ERS Task Force on Difficult/Therapy-Resistant Asthma. European Respiratory Society. Eur Respir J 1999;13:1198–1208. - PubMed
-
- Woolcock AJ. Corticosteroid-resistant asthma: definitions. Am J Respir Crit Care Med 1996;154:S45–S48. - PubMed
-
- Corrigan J, Brown PH, Barnes NC, Tsai J-J, Frew AJ, Kay AB. Glucocorticoid resistance in chronic asthma. Am Rev Respir Dis 1991;144:1016–1025. - PubMed
-
- Spahn JD, Landwehr LP, Nimmagadda S, Surs W, Leung DY, Szefler SJ. Effects of glucocorticoids on lymphocyte activation in patients with steroid-sensitive and steroid-resistant asthma. J Allergy Clin Immunol 1996;98:1073–1079. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
