

Segmental ulcerative vasculitis: a cutaneous manifestation of Takayasu's arteritis
- PMID: 16618320
- PMCID: PMC7951509
- DOI: 10.1111/j.1742-4801.2005.00103.x
Segmental ulcerative vasculitis: a cutaneous manifestation of Takayasu's arteritis
Abstract
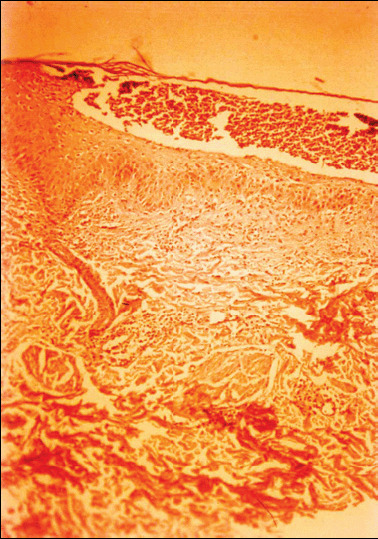
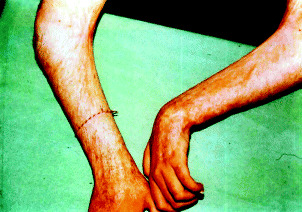
A 16-year-old girl with pyoderma gangrenosum (PG)-like skin lesions on the extremities, trunk and face developed Takayasu's arteritis (TA; pulseless disease). After 3 years under maintenance cyclosporin A therapy, the patient developed an ischaemic cerebral accident. Severe obstruction of both subclavian and left carotid arteries was found by Doppler sonography, angiography and computerised axial tomography. Evolution of this disease showed some characteristic findings: (a) PG-like lesions as the first cutaneous manifestation of pulseless disease; (b) methotrexate and cyclosporin A giving good results for the cutaneous lesions, but apparently not exerting an influence on the evolution of TA and the fatal outcome. This morphologic pattern may reflect underlying TA or Wegener's arteritis, and should be termed segmental ulcerative vasculitis.
Figures





Similar articles
-
Takayasu's disease with cutaneous involvement.Dermatology. 2004;208(1):10-5. doi: 10.1159/000075039. Dermatology. 2004. PMID: 14730230 Review.
-
Pyoderma gangrenosum associated with Takayasu's arteritis.Clin Exp Dermatol. 2004 Jul;29(4):357-9. doi: 10.1111/j.1365-2230.2004.01514.x. Clin Exp Dermatol. 2004. PMID: 15245528 Review.
-
Sarcoidosis as the initial manifestation of Takayasu's arteritis.J Med. 1994;25(1-2):121-8. J Med. 1994. PMID: 7930955
-
Pyoderma gangrenosum associated with Takayasu's arteritis responding to cyclosporin.Br J Dermatol. 1999 Aug;141(2):339-43. doi: 10.1046/j.1365-2133.1999.02989.x. Br J Dermatol. 1999. PMID: 10468813
-
Takayasu's arteritis coexisting with Wegener's granulomatosis in a teenager with renal insufficiency: case report.Pediatr Dev Pathol. 1999 Jul-Aug;2(4):385-8. doi: 10.1007/s100249900139. Pediatr Dev Pathol. 1999. PMID: 10347284
Cited by
-
Takayasu Arteritis.Front Pediatr. 2018 Sep 24;6:265. doi: 10.3389/fped.2018.00265. eCollection 2018. Front Pediatr. 2018. PMID: 30338248 Free PMC article. Review.
-
The Diagnostic Role of Skin Manifestations in Rheumatic Diseases in Children: A Critical Review of Paediatric Vasculitis.Int J Mol Sci. 2024 Jul 3;25(13):7323. doi: 10.3390/ijms25137323. Int J Mol Sci. 2024. PMID: 39000430 Free PMC article. Review.
-
Bulgarian rheumatology: science and practice in a cost-constrained environment.Rheumatol Int. 2019 Mar;39(3):417-429. doi: 10.1007/s00296-018-4202-2. Epub 2018 Nov 9. Rheumatol Int. 2019. PMID: 30413925 Review.
-
An unusual case of Takayasu arteritis presenting as isolated severe aortic regurgitation: A case report.Int J Surg Case Rep. 2023 Jul;108:108407. doi: 10.1016/j.ijscr.2023.108407. Epub 2023 Jun 15. Int J Surg Case Rep. 2023. PMID: 37356202 Free PMC article.
-
Numano type V Takayasu arteritis patients are more prone to have coronary artery involvement.Clin Rheumatol. 2020 Nov;39(11):3439-3447. doi: 10.1007/s10067-020-05123-2. Epub 2020 May 18. Clin Rheumatol. 2020. PMID: 32424657
References
-
- Perry HO, Winkelman RK, Miller SA et al. Malignant pyoderma. Arch Dermatol 1968; 98: 561–74. - PubMed
-
- Powell F, Winkelmann RK. Malignant pyoderma. Br J Dermatol 1983;109: 597–603. - PubMed
-
- Salassa JR, Winkelmann RK, McDonald TJ. Malignant pyoderma. Otolaryngol Head Neck Surg 1982;89: 917–22. - PubMed
-
- Lee CT, Thirumoorthy T. A case of malignant pyoderma with neurological manifestations. Ann Acad Med Singapore 1988;17: 554–56. - PubMed
-
- Gibson LE, Daoud MS, Muller SA, Perry HO. Malignant pyodermas revisited. Mayo Clin Proc 1997;72: 734–36. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
