

Review
doi: 10.1111/j.1365-2559.2006.02369.x.
Update on extranodal lymphomas. Conclusions of the Workshop held by the EAHP and the SH in Thessaloniki, Greece
Affiliations
- PMID: 16623775
- PMCID: PMC1448691
- DOI: 10.1111/j.1365-2559.2006.02369.x
Item in Clipboard
Review
Update on extranodal lymphomas. Conclusions of the Workshop held by the EAHP and the SH in Thessaloniki, Greece
Histopathology.
2006 Apr.
Abstract
Classification and proper treatment of extranodal lymphoma is hindered by the diversity of lymphoma types and the relative rarity of many of these tumour types. In order to review controversial issues in extranodal lymphoma diagnosis, a joint Workshop of the European Haematopathology Association (EAHP) and the Society for Hematopathology (SH) was held, where 99 selected cases were reviewed and discussed. This Workshop summary is focused on the most controversial aspect of cutaneous B-cell lymphoma, other extranodal B-cell lymphomas, plasmablastic lymphoma and anaplastic large-cell lymphoma in extranodal sites, and makes practical recommendations about diagnosis and therapeutic approaches.
Figures
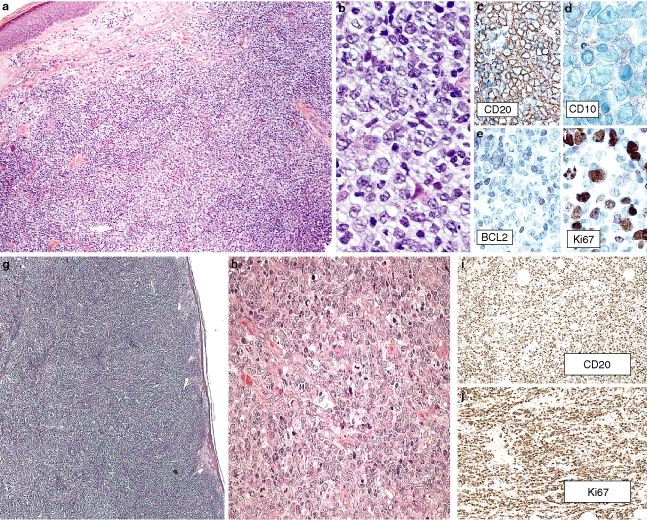
a–f, Primary cutaneous follicle centre lymphoma. a, Nodular pattern. b, Centroblastic predominance. c, CD20. d, CD10. e, Bcl-2. f, Ki67. g–j, Primary cutaneous diffuse large B-cell lymphoma, leg type. g,h, morphology, H&E. i, CD20. j, Ki67. Cases contributed by C. Girardet (A6) and R. S. Robertorye (A8).
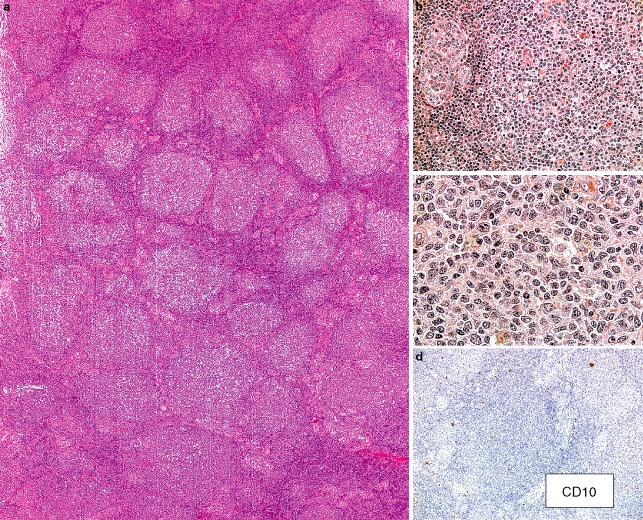
Follicular lymphoma of the thyroid. a, The thyroid in this 70-year-old male is extensively infiltrated by numerous lymphoid follicles with relatively homogeneous-appearing follicular/germinal centres. b, The interfollicular regions (left) adjacent to the neoplastic-appearing follicle demonstrate many small lymphocytes and prominent lymphoepithelial lesions. c, There are numerous small angulated lymphocytes with pale cytoplasm but only infrequent centroblasts in this follicular/germinal centre. (a–c, haematoxylin and eosin.) d, There are only scattered cells staining distinctly for CD10. Weak positivity was described in the case presentation. (CD10 immunostain with haematoxylin counterstain.) Other immunophenotypic studies were reported to show the following: CD20+, IgM–, IgD–, Bcl-6+, Bcl-2– and 50% Ki67 staining in the follicular structures. Polymerase chain reaction (PCR) studies did not demonstrate a clonal IGH rearrangement and neither PCR nor cytogenetic fluorescence in situ hybridization studies showed an IGH/BCL2 translocation. Case contributed by E. Navratil, A. Dogan, P. Isaacson.
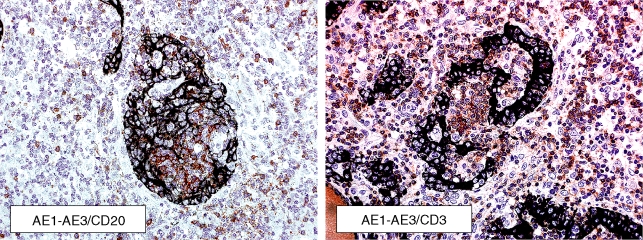
Classical Hodgkin lymphoma in thyroid. These double immunostains with the AE1/AE3 cytokeratin stain in black demonstrate that the lymphoepithelial lesions present in this case included some with many B cells (CD20 immunostain in red/brown on the left) and some with many T cells (CD3 immunostain in red/brown on the right). (Double immunostains with haematoxylin counterstain.) Case contributed by M. Vornanen.
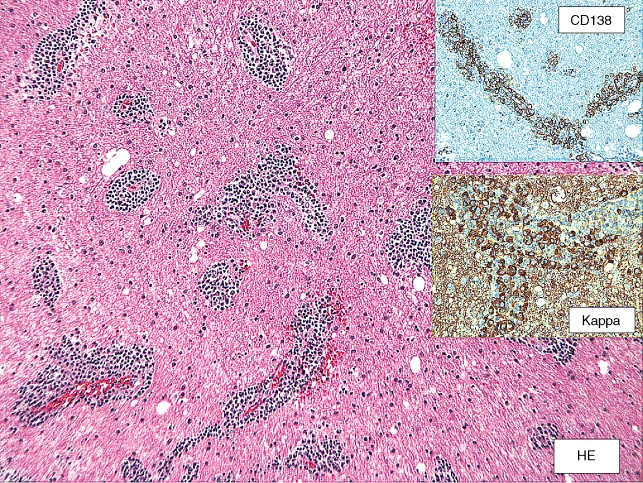
Lymphoplasmacytic lymphoma, primary in brain. Case contributed by E. Hsi (case B5).

Testicular follicular lymphoma, grade IIIa, t(14;18)–. Case contributed by C. Bacon and A. Dogan (case G6).
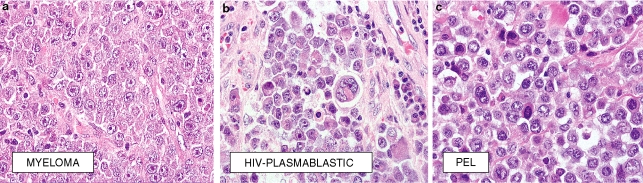
a, Extramedulary involvement by multiple myeloma. Case A11 contributed by F. Fend. b, Plasmablastic lymphoma with plasmacytic differentiation in a HIV+ patient. Case C12 contributed by J. Teruya-Feldstein. c, Primary effusion lymphoma presenting as a solid tumour. The tumour was positive for HHV8. Case C7 contributed by A. Dogan.
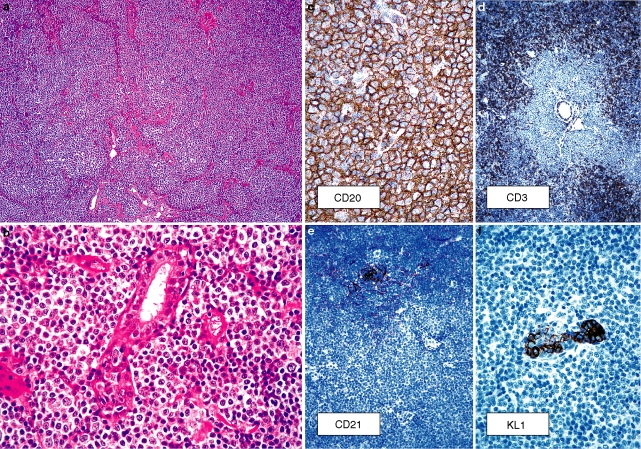
Marginal zone B-cell lymphoma in the breast. a,b, Morphology. c, CD20. d, CD3. e, CD21. f, KL1. Case contributed by F. Gaillard (D12).
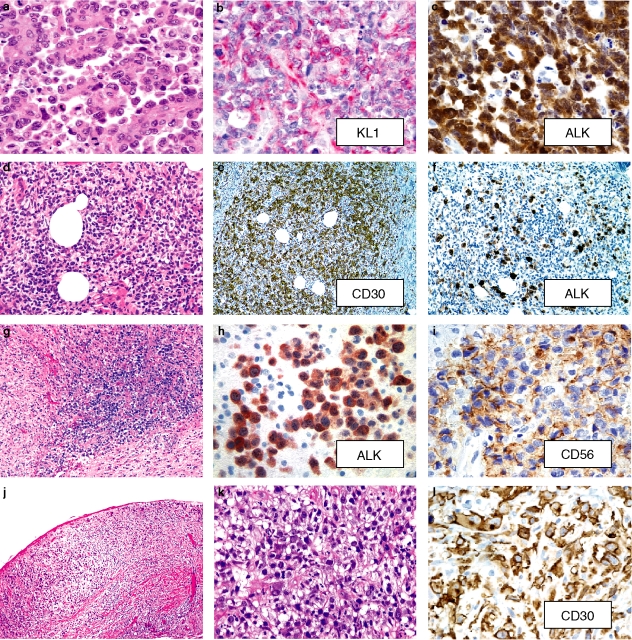
a–c, Keratin+ ALK+ anaplastic large-cell lymphoma in a pelvic mass from a 37-year-old female. a, The growth pattern suggests an epithelial process.b, The large cells strongly express pan keratin (KL1); epithelial membrane antigen is positive and CD45 and T-cell antigens and T-cell receptor gene rearrangements are negative (not shown). Ultrastructural features are compatible with lymphoma. c,
ALK present in the nucleus and cytoplasm. Case contributed by L. Donner, Temple, TX, USA (B4).
d–f,
ALK+ primary cutaneous anaplastic large-cell lymphoma presenting as a 30-mm tender thigh nodule in a 26-year-old male (Images case 89,A1). d, Sheets of large pleomorphic lymphocytes are present throughout the dermis. Many cells have a hallmark appearance with folded indented nuclei.e, The cells strongly express membrane and cytoplasmic (Golgi, dot-like) CD30. f, The cells have strong nuclear and cytoplasmic ALK expression. Fluorescence in situ hybridization studies confirmed translocation of the ALK gene. Careful staging and follow-up at 9 months showed no other evidence of disease. (Case contributed by B. Kim, Pittsburgh, PA, USA).g–i,
ALK+ primary CNS anaplastic large-cell lymphoma in a 27-year-old HIV– male (Images case 90,B9). g, Sheets of dysplastic large lymphocytes diffusely infiltrate the brain. h, The tumour cells have cytoplasmic and some nuclear ALK expression and are CD30+ (not shown). i, CD56 is present in the tumour cells. (Case contributed by Robert F. Bradley and Michael W. Beaty, Winston Salem, NC, USA.)j–k,
ALK– anaplastic large-cell lymphoma arising in the fibrous capsule surrounding a breast implant in a 49-year-old female (Images case 91,D11). k, Sheets of large tumour cells are present. l, The tumour cells are strongly CD30+ with a membrane and Golgi pattern of immunoreactivity. (Case contributed by Daphne de Jong, Amsterdam, the Netherlands).
Similar articles
-
The broad and challenging landscape of extranodal lymphoproliferations.Virchows Arch. 2020 May;476(5):633-646. doi: 10.1007/s00428-019-02702-w. Epub 2019 Nov 22. Virchows Arch. 2020. PMID: 31758317 Review.
-
Aggressive B-cell lymphomas: a review based on the workshop of the XI Meeting of the European Association for Haematopathology.Histopathology. 2005 Mar;46(3):241-55. doi: 10.1111/j.1365-2559.2005.02068.x. Histopathology. 2005. PMID: 15720410 Review.
-
[Peripheral NK/T-cell lymphoma].Pathologe. 2007 Feb;28(1):55-8. doi: 10.1007/s00292-006-0879-1. Pathologe. 2007. PMID: 17195040 German.
-
Lymphomas with plasmablastic features: a report of the lymphoma workshop of the 20th meeting of the European Association for Haematopathology.Virchows Arch. 2023 Nov;483(5):591-609. doi: 10.1007/s00428-023-03585-8. Epub 2023 Aug 10. Virchows Arch. 2023. PMID: 37561194
-
Extranodal lymphomas of the head and neck.Ann Diagn Pathol. 2005 Dec;9(6):340-50. doi: 10.1016/j.anndiagpath.2005.09.020. Ann Diagn Pathol. 2005. PMID: 16308165 Review.
Cited by
-
Early lesions in lymphoid neoplasia: Conclusions based on the Workshop of the XV. Meeting of the European Association of Hematopathology and the Society of Hematopathology, in Uppsala, Sweden.J Hematop. 2012 Sep;5(3):10.1007/s12308-012-0148-6. doi: 10.1007/s12308-012-0148-6. J Hematop. 2012. PMID: 24307917 Free PMC article.
-
Differentiating pulmonary cavities.Eur Respir Rev. 2013 Jun 1;22(128):191-2. doi: 10.1183/09059180.00005012. Eur Respir Rev. 2013. PMID: 23728876 Free PMC article. No abstract available.
-
The efficacy of HGAL and LMO2 in the separation of lymphomas derived from small B cells in nodal and extranodal sites, including the bone marrow.Am J Clin Pathol. 2011 May;135(5):697-708. doi: 10.1309/AJCP7Z2BIBUNQPLZ. Am J Clin Pathol. 2011. PMID: 21502424 Free PMC article.
-
Primary thyroid lymphoma: A case report and review of the literature.Ann Med Surg (Lond). 2016 Dec 21;13:29-33. doi: 10.1016/j.amsu.2016.12.023. eCollection 2017 Jan. Ann Med Surg (Lond). 2016. PMID: 28053701 Free PMC article.
-
Clinical significance of patterns of increased [18F]-FDG uptake in the thyroid gland: a pictorial review.Jpn J Radiol. 2018 Mar;36(3):181-193. doi: 10.1007/s11604-017-0715-y. Epub 2017 Dec 27. Jpn J Radiol. 2018. PMID: 29280068 Review.
References
-
- Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105:3768–3785. - PubMed
-
- Grange F, Petrella T, Beylot-Barry M, et al. Bcl-2 protein expression is the strongest independent prognostic factor of survival in primary cutaneous large B-cell lymphomas. Blood. 2004;103:3662–3668. - PubMed
-
- Vermeer MH, Geelen FA, van Haselen CW, et al. Primary cutaneous large B-cell lymphomas of the legs. A distinct type of cutaneous B-cell lymphoma with an intermediate prognosis. Dutch Cutaneous Lymphoma Working Group. Arch. Dermatol. 1996;132:1304–1308. - PubMed
-
- Geelen FA, Vermeer MH, Meijer CJ, et al. Bcl-2 protein expression in primary cutaneous large B-cell lymphoma is site-related. J. Clin. Oncol. 1998;16:2080–2085. - PubMed
-
- Grange F, Bekkenk MW, Wechsler J, et al. Prognostic factors in primary cutaneous large B-cell lymphomas: a European multicenter study. J. Clin. Oncol. 2001;19:3602–3610. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
