

Nuclear FABP7 immunoreactivity is preferentially expressed in infiltrative glioma and is associated with poor prognosis in EGFR-overexpressing glioblastoma
- PMID: 16623952
- PMCID: PMC1479358
- DOI: 10.1186/1471-2407-6-97
Nuclear FABP7 immunoreactivity is preferentially expressed in infiltrative glioma and is associated with poor prognosis in EGFR-overexpressing glioblastoma
Abstract
Background: We previously identified brain type fatty acid-binding protein (FABP7) as a prognostic marker for patients with glioblastoma (GBM). Increased expression of FABP7 is associated with reduced survival. To investigate possible molecular mechanisms underlying this association, we compared the expression and subcellular localization of FABP7 in non-tumor brain tissues with different types of glioma, and examined the expression of FABP7 and epidermal growth factor receptor (EGFR) in GBM tumors.
Methods: Expression of FABP7 in non-tumor brain and glioma specimens was examined using immunohistochemistry, and its correlation to the clinical behavior of the tumors was analyzed. We also analyzed the association between FABP7 and EGFR expression in different sets of GBM specimens using published DNA microarray datasets and semi-quantitative immunohistochemistry. In vitro migration was examined using SF763 glioma cell line.
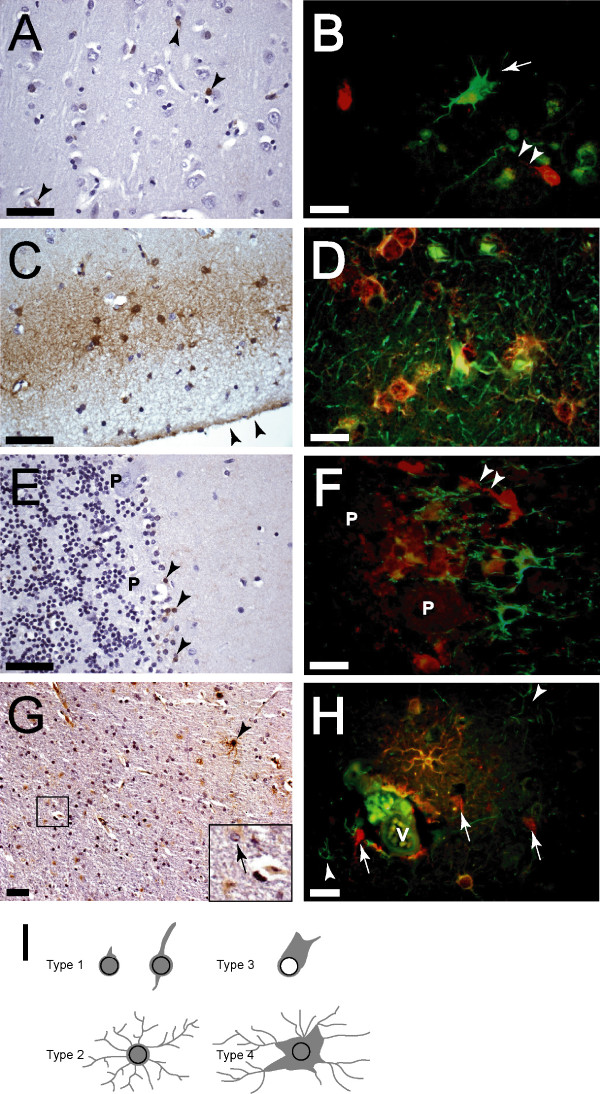
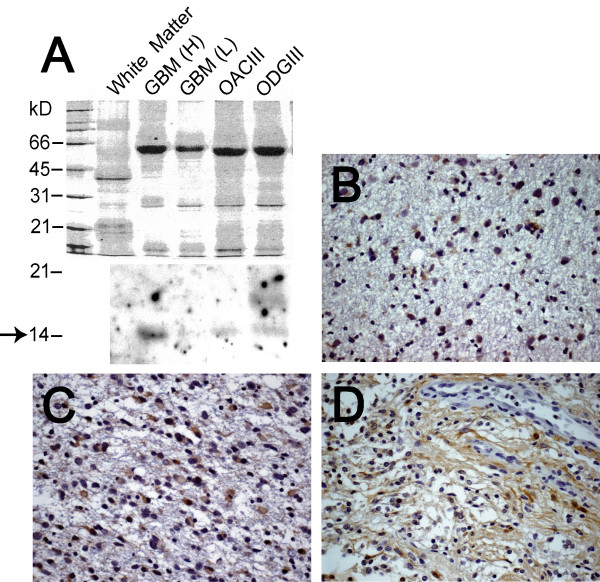
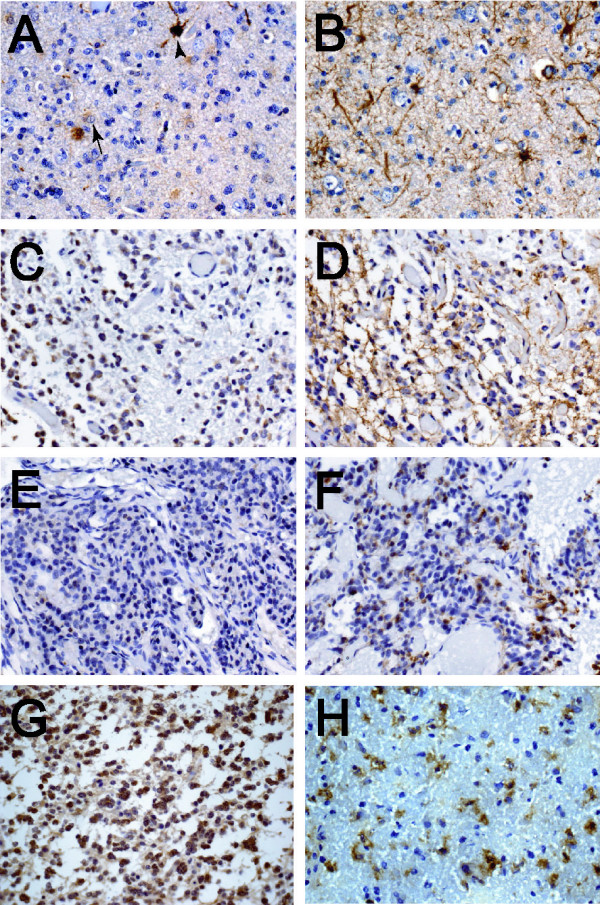
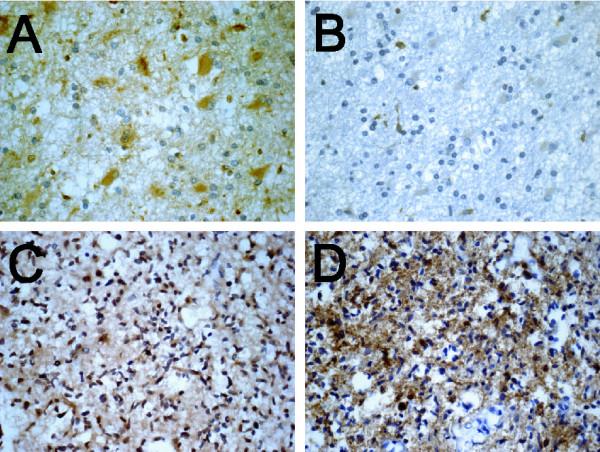
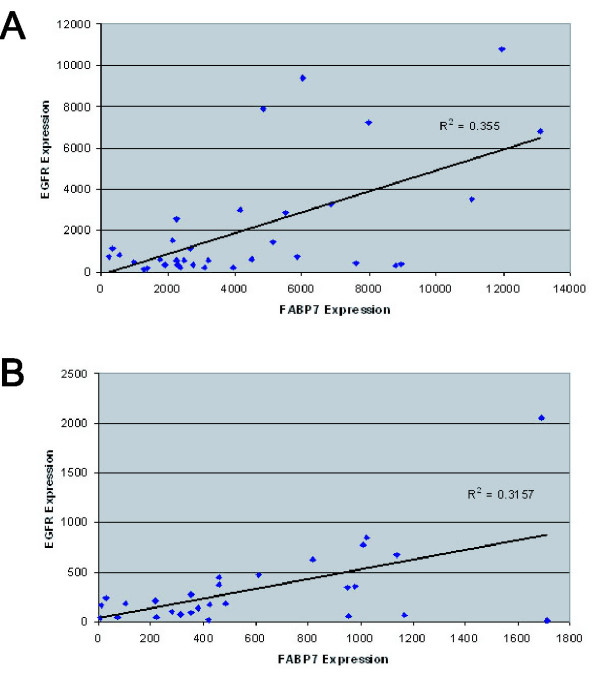
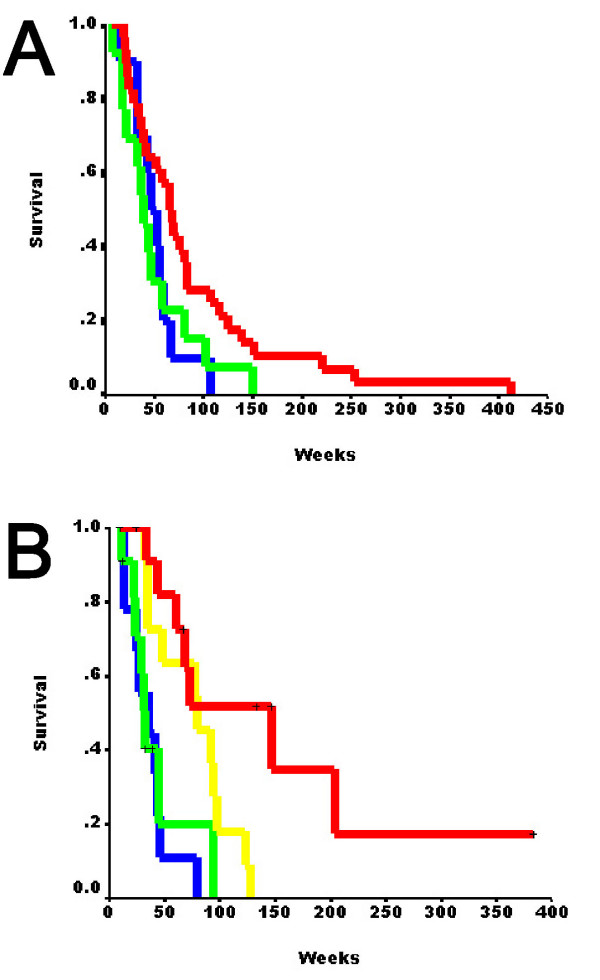
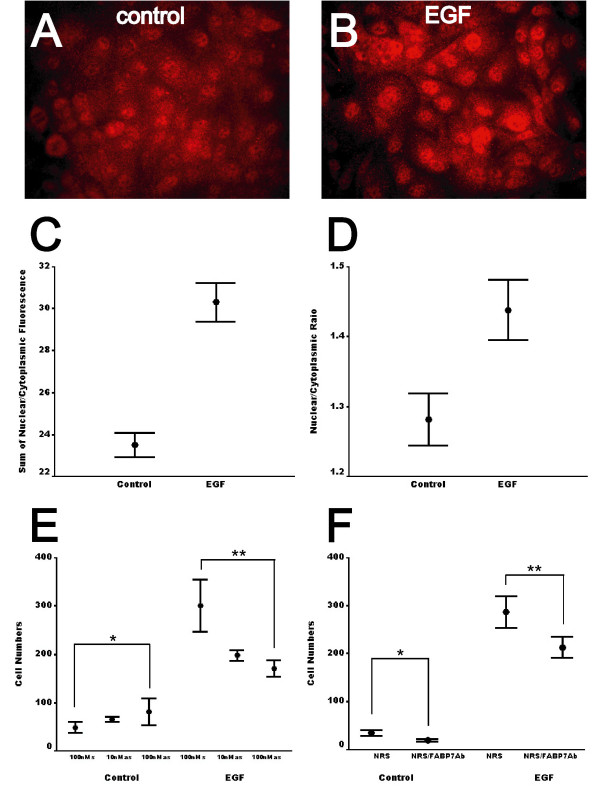
Results: FABP7 was present in a unique population of glia in normal human brain, and its expression was increased in a subset of reactive astrocytes. FABP7 immunoreactivity in grade I pilocytic astrocytoma was predominantly cytoplasmic, whereas nuclear FABP7 was detected in other types of infiltrative glioma. Nuclear, not cytoplasmic, FABP7 immunoreactivity was associated with EGFR overexpression in GBM (N = 61, p = 0.008). Expression of the FABP7 gene in GBM also correlated with the abundance of EGFR mRNA in our previous microarray analyses (N = 34, p = 0.016) and an independent public microarray dataset (N = 28, p = 0.03). Compared to those negative for both markers, nuclear FABP7-positive/EGFR-positive and nuclear FABP7-positive/EGFR-negative GBM tumors demonstrated shortest survival, whereas those only positive for EGFR had intermediate survival. EGFR activation increased nuclear FABP7 immunoreactivity in a glioma cell line in vitro, and inhibition of FABP7 expression suppressed EGF-induced glioma-cell migration. Our data suggested that in EGFR-positive GBM the presence of nuclear FABP7 immunoreactivity increases the risk of poor prognosis
Conclusion: In this study, we identified a possible mechanism as the basis of the association between nuclear FABP7 and poor prognosis of GBM. FABP7 expression can be found in all grades of astrocytoma, but neoplastic cells with nuclear FABP7 were only seen in infiltrative types of tumors. Nuclear FABP7 may be induced by EGFR activation to promote migration of GBM tumor cells. Positive nuclear FABP7 and EGFR overexpression correlated with short survival in EGFR-positive GBM patients. Therefore, nuclear FABP7 immunoreactivity could be used to monitor the progression of EGFR-overexpressed GBM.
Figures
References
-
- Medical Research Council Brain Tumor Working Party Randomized trial of procarbazine, lomustine, and vincristine in the adjuvant treatment of high-grade astrocytoma: a Medical Research Council trial. J Clin Oncol. 2001;19:509–518. - PubMed
-
- Korkolopoulou P, Christodoulou P, Kouzelis K, Hadjiyannakis M, Priftis A, Stamoulis G, Seretis A, Thomas-Tsagli E. MDM2 and p53 expression in gliomas: a multivariate survival analysis including proliferation markers and epidermal growth factor receptor. Br J Cancer. 1997;75:1269–1278. - PMC - PubMed
-
- Etienne MC, Formento JL, Lebrun-Frenay C, Gioanni J, Chatel M, Paquis P, Bernard C, Courdi A, Bensadoun RJ, Pignol JP, Francoual M, Grellier P, Frenay M, Milano G. Epidermal growth factor receptor and labeling index are independent prognostic factors in glial tumor outcome. Clin Cancer Res. 1998;4:2383–2390. - PubMed
-
- Waha A, Baumann A, Wolf HK, Fimmers R, Neumann J, Kindermann D, Astrahantseff K, Blumcke I, von Deimling A, Schlegel U. Lack of prognostic relevance of alterations in the epidermal growth factor receptor-transforming growth factor-alpha pathway in human astrocytic gliomas. J Neurosurg. 1996;85:634–641. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
