

Ultrasensitive monitoring of HIV-1 viral load by a low-cost real-time reverse transcription-PCR assay with internal control for the 5' long terminal repeat domain
- PMID: 16627558
- PMCID: PMC7108179
- DOI: 10.1373/clinchem.2006.066498
Ultrasensitive monitoring of HIV-1 viral load by a low-cost real-time reverse transcription-PCR assay with internal control for the 5' long terminal repeat domain
Abstract
Background: Current HIV-1 viral-load assays are too expensive for resource-limited settings. In some countries, monitoring of antiretroviral therapy is now more expensive than treatment itself. In addition, some commercial assays have shown shortcomings in quantifying rare genotypes.
Methods: We evaluated real-time reverse transcription-PCR with internal control targeting the conserved long terminal repeat (LTR) domain of HIV-1 on reference panels and patient samples from Brazil (n = 1186), South Africa (n = 130), India (n = 44), and Germany (n = 127).
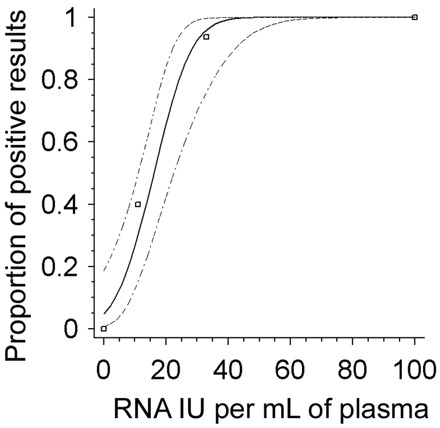
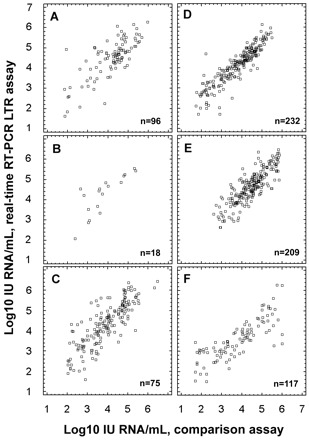
Results: The detection limit was 31.9 IU of HIV-1 RNA/mL of plasma (> 95% probability of detection, Probit analysis). The internal control showed inhibition in 3.7% of samples (95% confidence interval, 2.32%-5.9%; n = 454; 40 different runs). Comparative qualitative testing yielded the following: Roche Amplicor vs LTR assay (n = 431 samples), 51.7% vs 65% positives; Amplicor Ultrasensitive vs LTR (n = 133), 81.2% vs 82.7%; BioMerieux NucliSens HIV-1 QT (n = 453), 60.5% vs 65.1%; Bayer Versant 3.0 (n = 433), 57.7% vs 55.4%; total (n = 1450), 59.0% vs 63.8% positives. Intra-/interassay variability at medium and near-negative concentrations was 18%-51%. The quantification range was 50-10,000,000 IU/mL. Viral loads for subtypes A-D, F-J, AE, and AG yielded mean differences of 0.31 log(10) compared with Amplicor in the 10(3)-10(4) IU/mL range. HIV-1 N and O were not detected by Amplicor, but yielded up to 180 180.00 IU/mL in the LTR assay. Viral loads in stored samples from all countries, compared with Amplicor, NucliSens, or Versant, yielded regression line slopes (SD) of 0.9 (0.13) (P < 0.001 for all).
Conclusions: This method offers all features of commercial assays and covers all relevant genotypes. It could allow general monitoring of antiretroviral therapy in resource-limited settings.
Figures


Comment in
-
The battle against infectious diseases in developing countries: the inseparable twins of diagnosis and therapy.Clin Chem. 2006 Jul;52(7):1217. doi: 10.1373/clinchem.2006.071316. Clin Chem. 2006. PMID: 16798963 No abstract available.
References
-
- Valdiserri RO, Ogden LL, McCray E. Accomplishments in HIV prevention science: implications for stemming the epidemic. Nat Med 2003;9:881-886. - PubMed
-
- Ivers LC, Kendrick D, Doucette K. Efficacy of antiretroviral therapy programs in resource-poor settings: a meta-analysis of the published literature. Clin Infect Dis 2005;41:217-224. - PubMed
-
- Kaplan JE, Hanson DL, Jones JL, Dworkin MS. Viral load as an independent risk factor for opportunistic infections in HIV-infected adults and adolescents. AIDS 2001;15:1831-1836. - PubMed
-
- Hodinka RL. The clinical utility of viral quantitation using molecular methods. Clin Diagn Virol 1998;10:25-47. - PubMed
-
- Berger A, Braner J, Doerr HW, Weber B. Quantification of viral load: clinical relevance for human immunodeficiency virus, hepatitis B virus and hepatitis C virus infection. Intervirology 1998;41:24-34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
