

Endoscopic therapy for achalasia before Heller myotomy results in worse outcomes than heller myotomy alone
- PMID: 16632991
- PMCID: PMC1570551
- DOI: 10.1097/01.sla.0000217524.75529.2d
Endoscopic therapy for achalasia before Heller myotomy results in worse outcomes than heller myotomy alone
Abstract
Objective: Heller myotomy has been shown to be an effective primary treatment of achalasia. However, many physicians treating patients with achalasia continue to offer endoscopic therapies before recommending operative myotomy. Herein we report outcomes in 209 patients undergoing Heller myotomy with the majority (74%) undergoing myotomy as secondary treatment of achalasia.
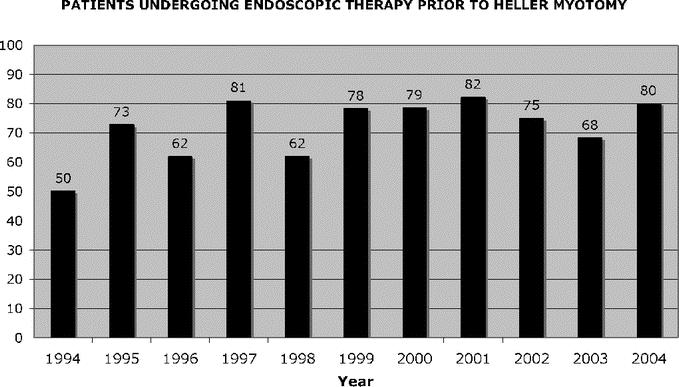
Methods: Data on all patients undergoing operative management of achalasia are collected prospectively. Over a 9-year period (1994-2003), 209 patients underwent Heller myotomy for achalasia. Of these, 154 had undergone either Botox injection and/or pneumatic dilation preoperatively. Preoperative, operative, and long-term outcome data were analyzed. Statistical analysis was performed with multiple chi and Mann-Whitney U analyses, as well as ANOVA.
Results: Among the 209 patients undergoing Heller myotomy for achalasia, 154 received endoscopic therapy before being referred for surgery (100 dilation only, 33 Botox only, 21 both). The groups were matched for preoperative demographics and symptom scores for dysphagia, regurgitation, and chest pain. Intraoperative complications were more common in the endoscopically treated group with GI perforations being the most common complication (9.7% versus 3.6%). Postoperative complications, primarily severe dysphagia, and pulmonary complications were more common after endoscopic treatment (10.4% versus 5.4%). Failure of myotomy as defined by persistent or recurrent severe symptoms, or need for additionally therapy including redo myotomy or esophagectomy was higher in the endoscopically treated group (19.5% versus 10.1%).
Conclusion: Use of preoperative endoscopic therapy remains common and has resulted in more intraoperative complications, primarily perforation, more postoperative complications, and a higher rate of failure than when no preoperative therapy was used. Endoscopic therapy for achalasia should not be used unless patients are not candidates for surgery.
Figures
Comment in
-
Reflux after Heller's myotomy for achalasia.Ann Surg. 2007 Mar;245(3):502-3. doi: 10.1097/01.sla.0000256108.41616.32. Ann Surg. 2007. PMID: 17435559 Free PMC article. No abstract available.
References
-
- Bonavina L, Nosadini A, Bardini R, et al. Primary treatment of esophageal achalasia: long-term results of myotomy and Dor fundoplication. Arch Surg. 1992;127:222–226; discussion 227. - PubMed
-
- Ellis FH Jr, Crozier RE, Watkins E Jr. Operation for esophageal achalasia: results of esophagomyotomy without an antireflux operation. J Thorac Cardiovasc Surg. 1984;88:344–351. - PubMed
-
- Okike N, Payne WS, Neufeld DM, et al. Esophagomyotomy versus forceful dilation for achalasia of the esophagus: results in 899 patients. Ann Thorac Surg. 1979;28:119–125. - PubMed
-
- Pinotti HW, Sakai P, Ishioka S. Cardiomyotomy and fundoplication for esophageal achalasia. Jpn J Surg. 1983;13:399–403. - PubMed
-
- Bonatti H, Hinder RA, Klocker J, et al. Long-term results of laparoscopic Heller myotomy with partial fundoplication for the treatment of achalasia. Am J Surg. 2006;190:874–878. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
