

Intermediate-term outcomes with expanded criteria deceased donors in kidney transplantation: a spectrum or specter of quality?
- PMID: 16632993
- PMCID: PMC1570560
- DOI: 10.1097/01.sla.0000216302.43776.1a
Intermediate-term outcomes with expanded criteria deceased donors in kidney transplantation: a spectrum or specter of quality?
Abstract
Objective: To compare intermediate-term outcomes in adult recipients of expanded criteria (ECD) versus concurrent standard criteria (SCD) deceased donor kidney transplants at a single center using a standardized approach.
Summary background data: Expanded criteria donors (ECDs) are a source of kidneys that increase the donor organ pool, but the value of transplanting these kidneys has been questioned because of concerns regarding diminished survival and predicted poorer intermediate-term outcomes.
Methods: Over a 47-month period, we performed 244 deceased donor kidney transplants into adult recipients, including 143 from SCDs and 101 from ECDs. Management algorithms were implemented to preserve nephron function, and recipient selection for an ECD kidney transplant was based on low immunologic risk. All patients received depleting antibody induction in combination with tacrolimus and mycophenolate mofetil. A total of 188 patients (77%) had at least a 1-year follow-up.
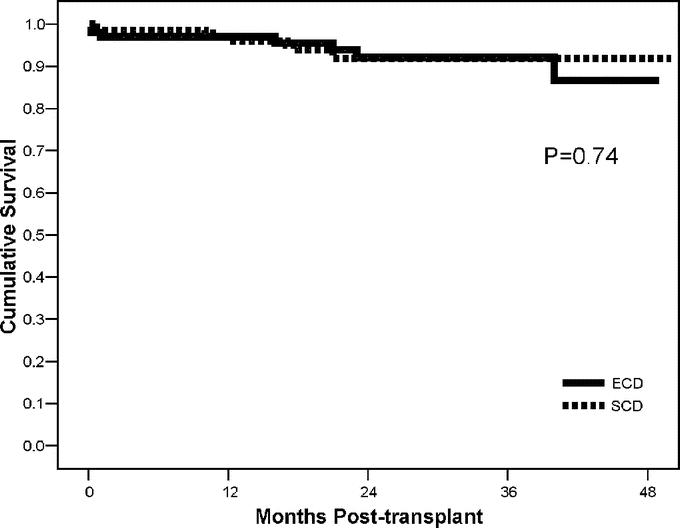
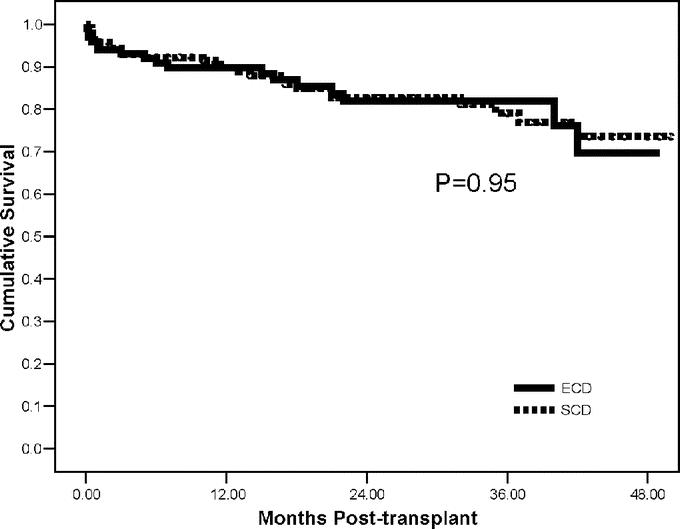
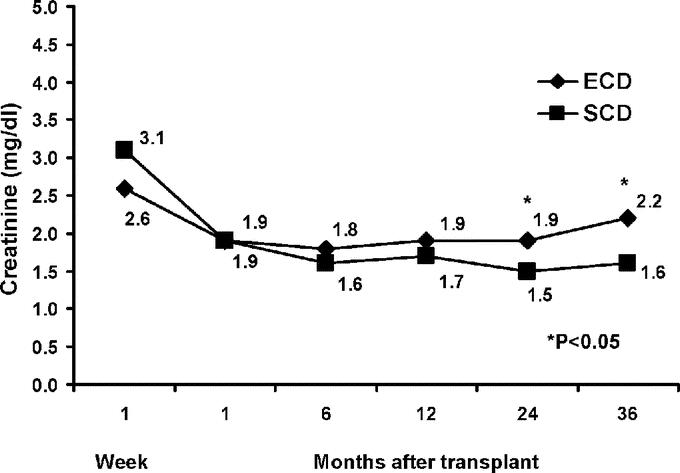
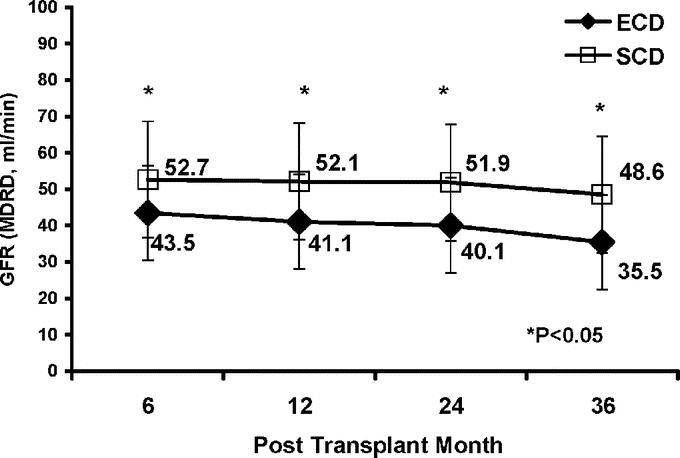
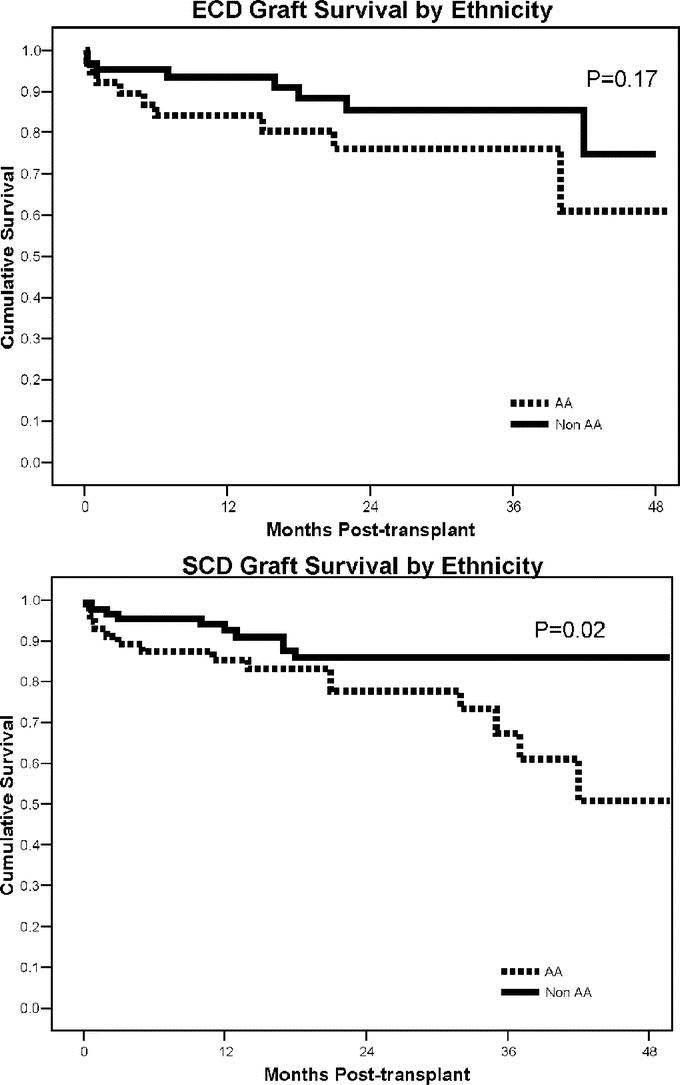
Results: ECDs were older, had a higher BMI, had an increased incidence of cerebrovascular brain death and preexisting donor hypertension, and had a lower estimated creatinine clearance (CrCl, all P < 0.01) compared with SCDs. Cold ischemic times were similar between groups, but more ECD kidneys were preserved with pulsatile perfusion (P < 0.01). ECD kidney recipients were older, less sensitized, had a lower BMI, had fewer 0-antigen mismatches, and had a shorter waiting time (all P < 0.01) compared with SCD kidney recipients. Actual patient (93%) and kidney graft (83%) survival rates were similar between groups with a mean follow-up of 24 months. The rates of delayed graft function (DGF), acute rejection, readmissions, operative complications, major infections, and resource utilization were comparable between groups. Renal function followed longitudinally was consistently better in SCD patients (P < 0.05). Black recipients had higher rates of DGF, acute rejection, and graft loss (P < 0.05), but the effects were less pronounced in the ECD group.
Conclusions: By appropriate donor and recipient profiling and the use of management algorithms to project and protect renal function, excellent intermediate-term outcomes can be achieved with ECD kidney transplants that are comparable to SCD kidney transplants.
Figures
Similar articles
-
Long-term outcomes of kidney transplantation from expanded criteria deceased donors at a single center: comparison with standard criteria deceased donors.Transplant Proc. 2014;46(2):431-6. doi: 10.1016/j.transproceed.2013.11.061. Transplant Proc. 2014. PMID: 24655981
-
Dual kidney transplants from adult marginal donors successfully expand the limited deceased donor organ pool.Clin Transplant. 2016 Apr;30(4):380-92. doi: 10.1111/ctr.12697. Epub 2016 Feb 15. Clin Transplant. 2016. PMID: 26782941
-
Impact of acute kidney injury in expanded criteria deceased donors on post-transplant clinical outcomes: multicenter cohort study.BMC Nephrol. 2019 Feb 4;20(1):39. doi: 10.1186/s12882-019-1225-1. BMC Nephrol. 2019. PMID: 30717699 Free PMC article.
-
Single center experience and literature review of kidney transplantation from non-ideal donors with acute kidney injury: Risk and reward.Clin Transplant. 2023 Oct;37(10):e15115. doi: 10.1111/ctr.15115. Epub 2023 Aug 30. Clin Transplant. 2023. PMID: 37646473 Review.
-
Long-term outcomes of kidney transplantation from deceased donors with terminal acute kidney injury: Single center experience and literature review.Clin Transplant. 2023 Mar;37(3):e14886. doi: 10.1111/ctr.14886. Epub 2022 Dec 28. Clin Transplant. 2023. PMID: 36524320 Review.
Cited by
-
A Retrospective Cohort Study on Rehospitalization following Expanded Criteria Donor Kidney Transplantation.Surg Res Pract. 2018 Dec 25;2018:4879850. doi: 10.1155/2018/4879850. eCollection 2018. Surg Res Pract. 2018. PMID: 30675510 Free PMC article.
-
Single vs dual (en bloc) kidney transplants from donors ≤ 5 years of age: A single center experience.World J Transplant. 2016 Mar 24;6(1):239-48. doi: 10.5500/wjt.v6.i1.239. World J Transplant. 2016. PMID: 27011923 Free PMC article.
-
Delayed graft function and the risk of acute rejection in the modern era of kidney transplantation.Kidney Int. 2015 Oct;88(4):851-8. doi: 10.1038/ki.2015.190. Epub 2015 Jun 24. Kidney Int. 2015. PMID: 26108067
-
Implications of donor disseminated intravascular coagulation on kidney allograft recipients.Clin J Am Soc Nephrol. 2011 May;6(5):1160-7. doi: 10.2215/CJN.07280810. Epub 2011 Mar 3. Clin J Am Soc Nephrol. 2011. PMID: 21372214 Free PMC article.
-
Opportunities and challenges of expanded criteria organs in liver and kidney transplantation as a response to organ shortage.Mo Med. 2011 Jul-Aug;108(4):269-74. Mo Med. 2011. PMID: 21905444 Free PMC article.
References
-
- United Network for Organ Sharing. National data. Available at: http://www.unos.org/data. Accessed November 17, 2005.
-
- Rosendale JD. Organ donation in the United States: 1988–2002. In: Cecka JM, Terasaki PI, eds. Clinical Transplantation 2003. Los Angeles: UCLA Immunogenetics Center, 2004:65–76.
-
- Nathan HM, Conrad SL, Held PJ, et al. Organ donation in the United States. Am J Transplant. 2003;3(suppl. 4):29–40. - PubMed
-
- Metzger RA, Delmonico FL, Feng S, et al. Expanded criteria donors for kidney transplantation. Am J Transplant. 2003;3(suppl 4):114–125. - PubMed
-
- Ojo AO, Hanson JA, Meier-Kriesche H, et al. Survival in recipients of marginal cadaveric donor kidneys compared with other recipients and wait-listed transplant candidates. J Am Soc Nephrol. 2001;12:589–597. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
