

Early identification of intensive care unit-acquired infections with daily monitoring of C-reactive protein: a prospective observational study
- PMID: 16635270
- PMCID: PMC1550913
- DOI: 10.1186/cc4892
Early identification of intensive care unit-acquired infections with daily monitoring of C-reactive protein: a prospective observational study
Abstract
Introduction: Manifestations of sepsis are sensitive but are poorly specific of infection. Our aim was to assess the value of daily measurements of C-reactive protein (CRP), temperature and white cell count (WCC) in the early identification of intensive care unit (ICU)-acquired infections.
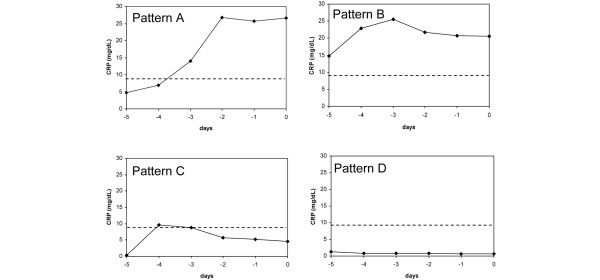
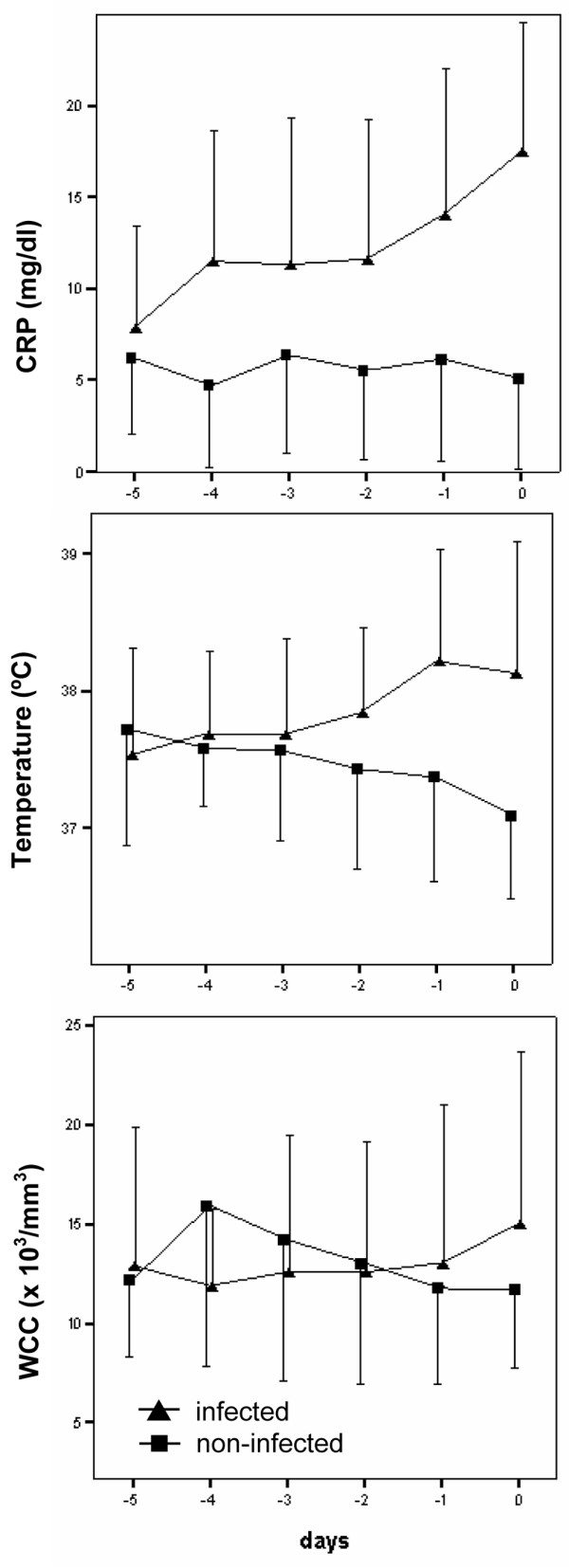
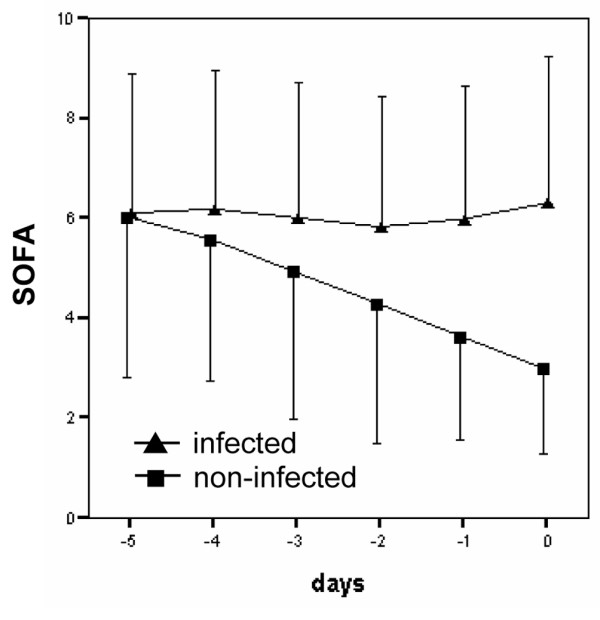
Methods: We undertook a prospective observational cohort study (14 month). All patients admitted for > or =72 hours (n = 181) were divided into an infected (n = 35) and a noninfected group (n = 28). Infected patients had a documented ICU-acquired infection and were not receiving antibiotics for at least 5 days before diagnosis. Noninfected patients never received antibiotics and were discharged alive. The progression of CRP, temperature and WCC from day -5 to day 0 (day of infection diagnosis or of ICU discharge) was analyzed. Patients were divided into four patterns of CRP course according to a cutoff value for infection diagnosis of 8.7 mg/dl: pattern A, day 0 CRP >8.7 mg/dl and, in the previous days, at least once below the cutoff; pattern B, CRP always >8.7 mg/dl; pattern C, day 0 CRP < or =8.7 mg/dl and, in the previous days, at least once above the cutoff; and pattern D, CRP always < or =8.7 mg/dl.
Results: CRP and the temperature time-course showed a significant increase in infected patients, whereas in noninfected it remained almost unchanged (P < 0.001 and P < 0.001, respectively). The area under the curve for the maximum daily CRP variation in infection prediction was 0.86 (95% confidence interval: 0.752-0.933). A maximum daily CRP variation >4.1 mg/dl was a good marker of infection prediction (sensitivity 92.1%, specificity 71.4%), and in combination with a CRP concentration >8.7 mg/dl the discriminative power increased even further (sensitivity 92.1%, specificity 82.1%). Infection was diagnosed in 92% and 90% of patients with patterns A and B, respectively, and in only two patients with patterns C and D (P < 0.001).
Conclusion: Daily CRP monitoring and the recognition of the CRP pattern could be useful in the prediction of ICU-acquired infections. Patients presenting maximum daily CRP variation >4.1 mg/dl plus a CRP level >8.7 mg/dl had an 88% risk of infection.
Figures
References
-
- Brun-Buisson C, Doyon F, Carlet J, Dellamonica P, Gouin F, Lepoutre A, Mercier JC, Offenstadt G, Regnier B. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA. 1995;274:968–974. doi: 10.1001/jama.274.12.968. - DOI - PubMed
-
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20:864–874. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
