

Where tendons and ligaments meet bone: attachment sites ('entheses') in relation to exercise and/or mechanical load
- PMID: 16637873
- PMCID: PMC2100202
- DOI: 10.1111/j.1469-7580.2006.00540.x
Where tendons and ligaments meet bone: attachment sites ('entheses') in relation to exercise and/or mechanical load
Abstract
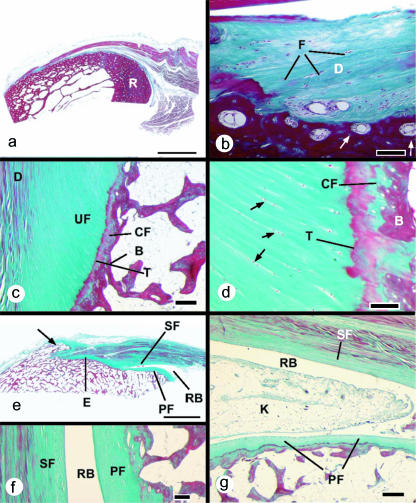
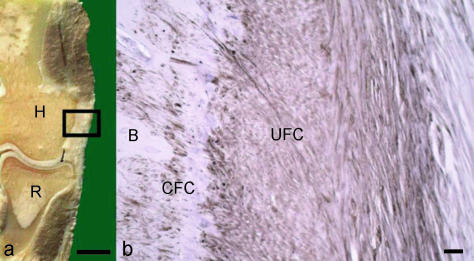
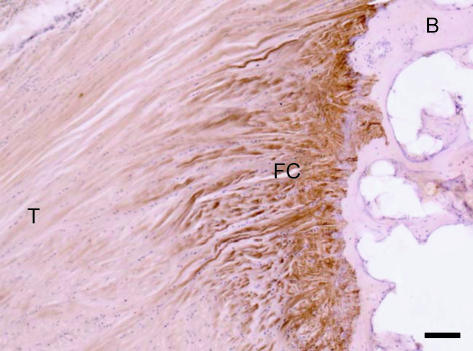
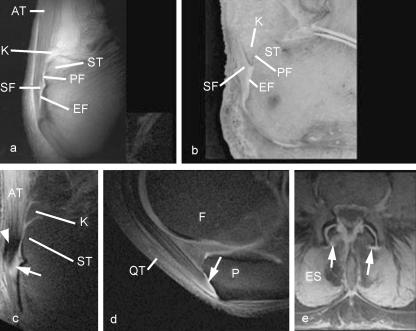
Entheses (insertion sites, osteotendinous junctions, osteoligamentous junctions) are sites of stress concentration at the region where tendons and ligaments attach to bone. Consequently, they are commonly subject to overuse injuries (enthesopathies) that are well documented in a number of sports. In this review, we focus on the structure-function correlations of entheses on both the hard and the soft tissue sides of the junction. Particular attention is paid to mechanical factors that influence form and function and thus to exploring the relationship between entheses and exercise. The molecular parameters indicative of adaptation to mechanical stress are evaluated, and the basis on which entheses are classified is explained. The application of the 'enthesis organ' concept (a collection of tissues adjacent to the enthesis itself, which jointly serve the common function of stress dissipation) to understanding enthesopathies is considered and novel roles of adipose tissue at entheses are reviewed. A distinction is made between different locations of fat at entheses, and possible functions include space-filling and proprioception. The basic anchorage role of entheses is considered in detail and comparisons are explored between entheses and other biological 'anchorage' sites. The ability of entheses for self-repair is emphasized and a range of enthesopathies common in sport are reviewed (e.g. tennis elbow, golfer's elbow, jumper's knee, plantar fasciitis and Achilles insertional tendinopathies). Attention is drawn to the degenerative, rather than inflammatory, nature of most enthesopathies in sport. The biomechanical factors contributing to the development of enthesopathies are reviewed and the importance of considering the muscle-tendon-bone unit as a whole is recognized. Bony spur formation is assessed in relation to other changes at entheses which parallel those in osteoarthritic synovial joints.
Figures
References
-
- Abreu MR, Chung CB, Mendes L, Mohana-Borges A, Trudell D, Resnick D. Plantar calcaneal enthesophytes: new observations regarding sites of origin based on radiographic, MR imaging, anatomic, and paleopathologic analysis. Skeletal Radiol. 2003;32:13–21. - PubMed
-
- Adams CMW, Bayliss OB, Baker RWR, Abdulla YH, Huntercraig CJ. Lipid deposits in aging human arteries, tendons, and fascia. Atherosclerosis. 1974;19:429–440. - PubMed
-
- Andriacchi TP, Birac D. Functional testing in the anterior cruciate ligament-deficient knee. Clin Orthop Relat Res. 1993;288:40–47. - PubMed
-
- Aoki M, Oguma H, Fukushima S, Ishii S, Ohtani S, Murakami G. Fibrous connection to bone after immediate repair of the canine infraspinatus: the most effective bony surface for tendon attachment. J Shoulder Elbow Surg. 2001;10:123–128. - PubMed
-
- Bell E, Gosline J. Mechanical design of mussel byssus: material yield enhances attachment strength. J Exp Biol. 1996;199:1005–1017. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
