

The effects of exercise on human articular cartilage
- PMID: 16637874
- PMCID: PMC2100201
- DOI: 10.1111/j.1469-7580.2006.00546.x
The effects of exercise on human articular cartilage
Abstract
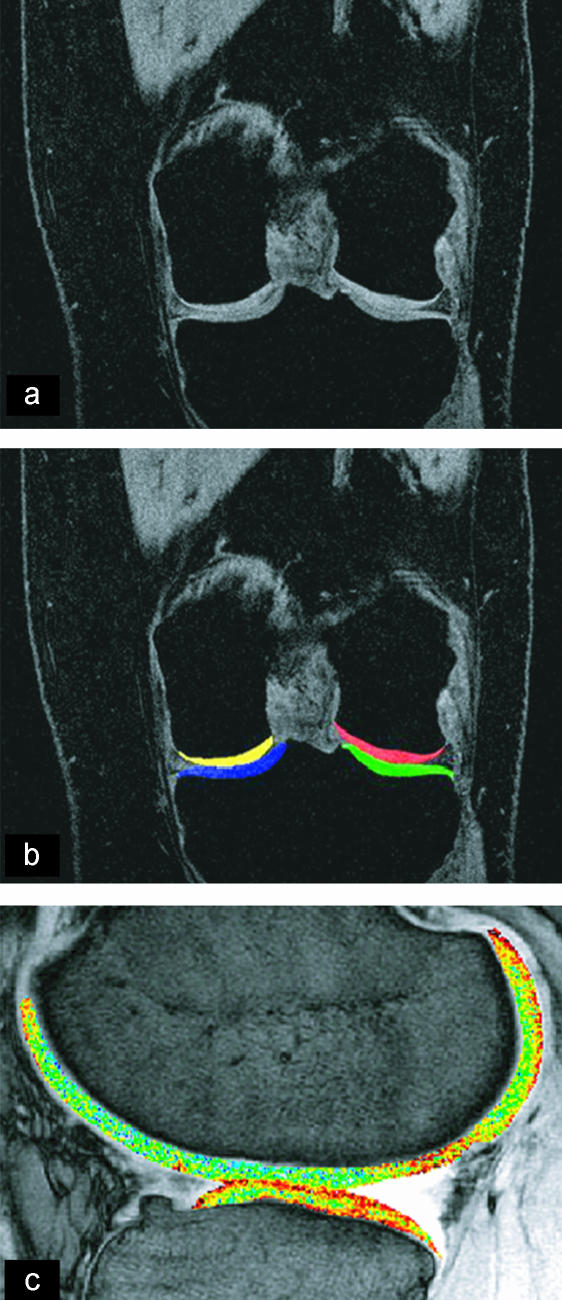
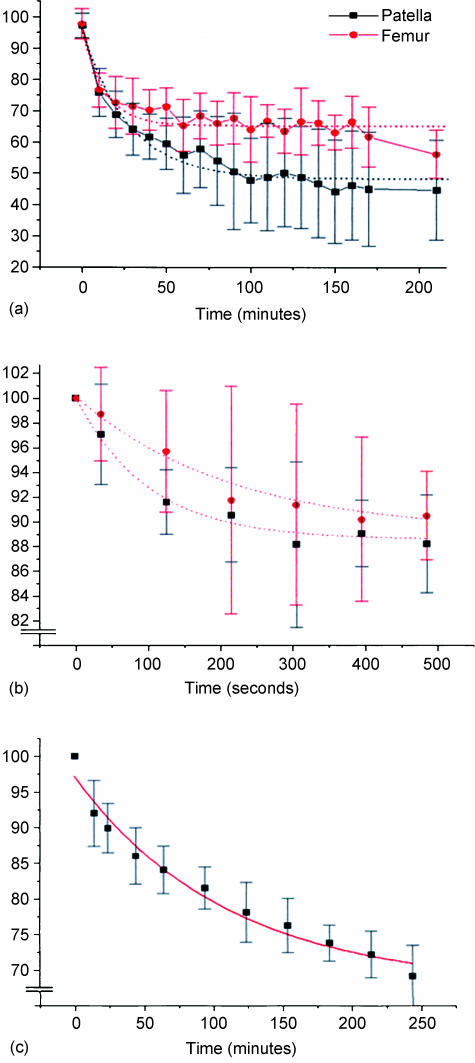
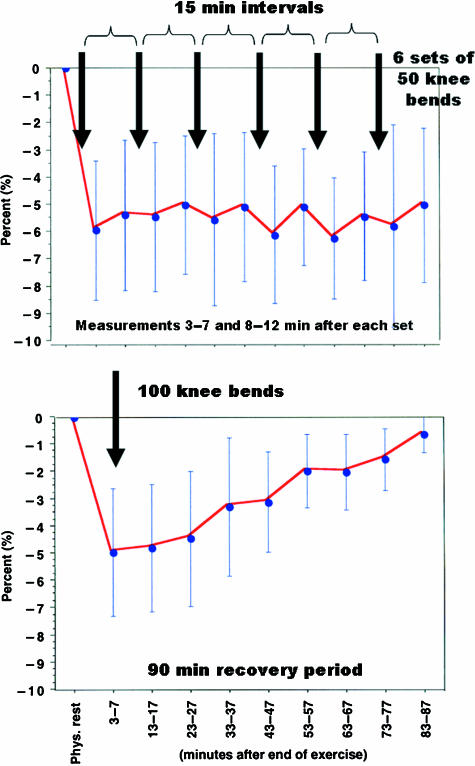
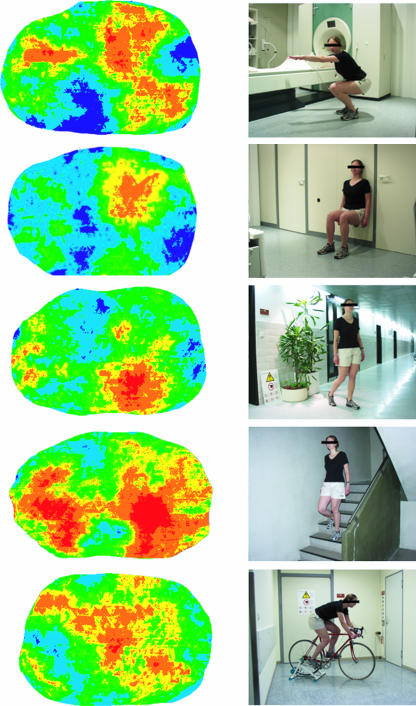
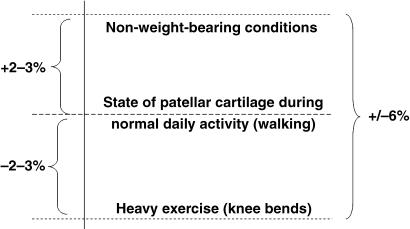
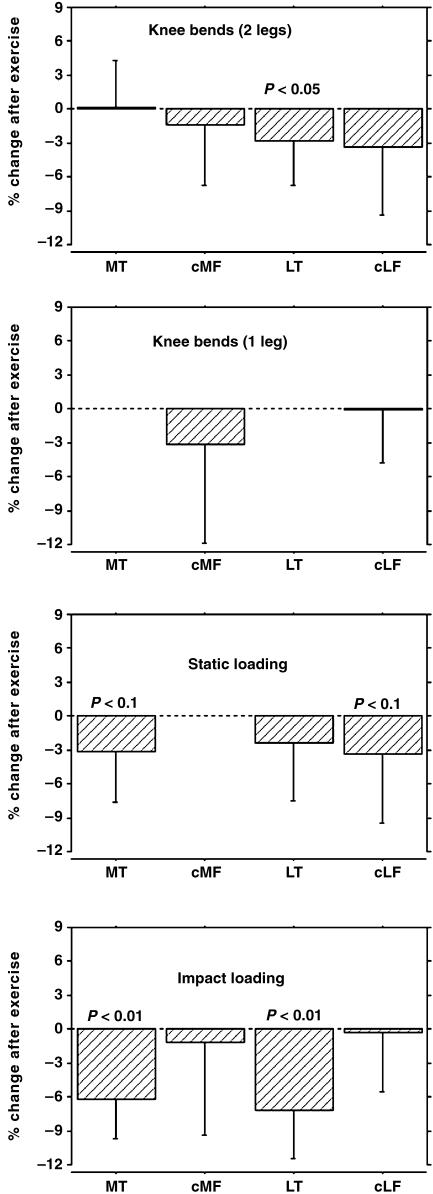
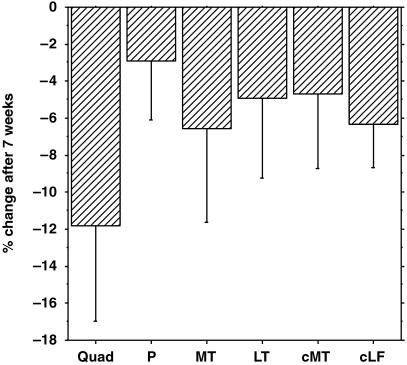
The effects of exercise on articular hyaline articular cartilage have traditionally been examined in animal models, but until recently little information has been available on human cartilage. Magnetic resonance imaging now permits cartilage morphology and composition to be analysed quantitatively in vivo. This review briefly describes the methodological background of quantitative cartilage imaging and summarizes work on short-term (deformational behaviour) and long-term (functional adaptation) effects of exercise on human articular cartilage. Current findings suggest that human cartilage deforms very little in vivo during physiological activities and recovers from deformation within 90 min after loading. Whereas cartilage deformation appears to become less with increasing age, sex and physical training status do not seem to affect in vivo deformational behaviour. There is now good evidence that cartilage undergoes some type of atrophy (thinning) under reduced loading conditions, such as with postoperative immobilization and paraplegia. However, increased loading (as encountered by elite athletes) does not appear to be associated with increased average cartilage thickness. Findings in twins, however, suggest a strong genetic contribution to cartilage morphology. Potential reasons for the inability of cartilage to adapt to mechanical stimuli include a lack of evolutionary pressure and a decoupling of mechanical competence and tissue mass.
Figures


References
-
- Al Ali D, Graichen H, Faber S, et al. Quantitative cartilage imaging of the human hind foot: precision and inter-subject variability. J Orthop Res. 2002;20:249–256. - PubMed
-
- Antoniades L, Spector TD, MacGregor AJ. The genetic contribution to hip joint morphometry and relationship to hip cartilage thickness. Osteoarthritis Cartilage. 2001;9:593–595. - PubMed
-
- Ateshian GA, Soslowsky LJ, Mow VC. Quantitation of articular surface topography and cartilage thickness in knee joints using stereophotogrammetry. J Biomech. 1991;24:761–776. - PubMed
-
- Ateshian GA, Lai WM, Zhu WB, Mow VC. An asymptotic solution for the contact of two biphasic cartilage layers. J Biomech. 1994;27:1347–1360. - PubMed
-
- Ateshian G, Mow VC. Friction, lubrication, and wear of articular cartilage and diathrodial joints. In: Mow VC, Huskes R, editors. Basic Orthopaedic Biomechanics and Mechanobiology. 3. Philadelphia: Lippincott, Williams & Wilkins; 2005. pp. 447–494.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
