

Using the six sigma process to implement the Centers for Disease Control and Prevention Guideline for Hand Hygiene in 4 intensive care units
- PMID: 16637959
- PMCID: PMC2557134
- DOI: 10.1111/j.1525-1497.2006.00361.x
Using the six sigma process to implement the Centers for Disease Control and Prevention Guideline for Hand Hygiene in 4 intensive care units
Abstract
Background: The Centers for Disease Control and Prevention (CDC) Guideline for Hand Hygiene in Health Care Settings was issued in 2002. In 2003, the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) established complying with the CDC Guideline as a National Patient Safety Goal for 2004. This goal has been maintained through 2006. The CDC's emphasis on the use of alcohol-based hand rubs (ABHRs) rather than soap and water was an opportunity to improve compliance, but the Guideline contained over 40 specific recommendations to implement.
Objective: To use the Six Sigma process to examine hand hygiene practices and increase compliance with the CDC hand hygiene recommendations required by JCAHO.
Design: Six Sigma Project with pre-post design.
Participants: Physicians, nurses, and other staff working in 4 intensive care units at 3 hospitals.
Measurements: Observed compliance with 10 required hand hygiene practices, mass of ABHR used per month per 100 patient-days, and staff attitudes and perceptions regarding hand hygiene reported by questionnaire.
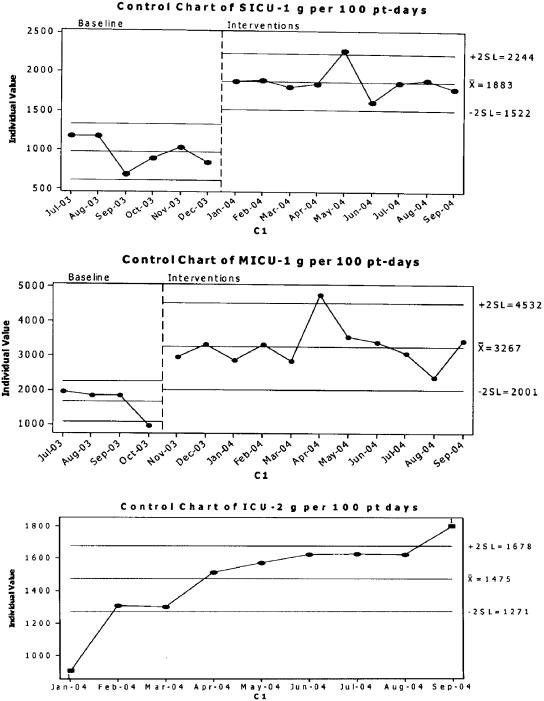
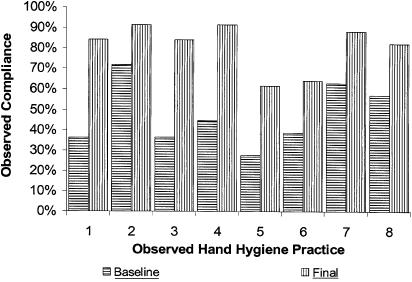
Results: Observed compliance increased from 47% to 80%, based on over 4,000 total observations. The mass of ABHR used per 100 patient-days in 3 intensive care units (ICUs) increased by 97%, 94%, and 70%; increases were sustained for 9 months. Self-reported compliance using the questionnaire did not change. Staff reported increased use of ABHR and increased satisfaction with hand hygiene practices and products.
Conclusions: The Six Sigma process was effective for organizing the knowledge, opinions, and actions of a group of professionals to implement the CDC's evidence-based hand hygiene practices in 4 ICUs. Several tools were developed for widespread use.
Figures
References
-
- Semmelweis I. In: Etiology, Concept, and Prophylaxis of Childbed Fever. 1. Carter KC, editor. Madison, WI: The University of Wisconsin Press; 1983.
-
- Institute of Medicine. Priority Areas for National Action. Washington, DC: National Academies Press; 2003. - PubMed
-
- Boyce JM. MRSA patients: proven methods to treat colonization. J Hosp Infect. 2001;48(suppl A):S9–14. - PubMed
-
- Larson E. Skin hygiene and infection prevention: more of the same or different approaches? Clin Infec Dis. 1999;29:1287–94. - PubMed
-
- Leape LL, Brennan TA, Laird N, et al. The nature of adverse events in hospitalized patients. N Engl J Med. 1991;324:377–84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical