

Urgent GP referrals for suspected lung, colorectal, prostate and ovarian cancer
- PMID: 16638251
- PMCID: PMC1837844
Urgent GP referrals for suspected lung, colorectal, prostate and ovarian cancer
Abstract
Background: The UK urgent cancer referral guidance was introduced between 1999-2000. There is a dearth of literature relating to the effectiveness in detecting cancer of urgent suspected cancer referrals and general practitioners' compliance with the guidance.
Aims: This paper aims to determine the diagnostic yield from urgent referrals for suspected colorectal, lung, ovarian and prostate cancer, and the proportion of patients with cancer who were urgently referred. Secondary aims are to determine the association of these findings with age, ethnicity, sex and marital status, and to determine the proportions of patients who fulfilled the urgent referral criteria.
Design: Detailed notes analysis of all urgent referrals and all cancer diagnoses.
Setting: One hospital trust in England.
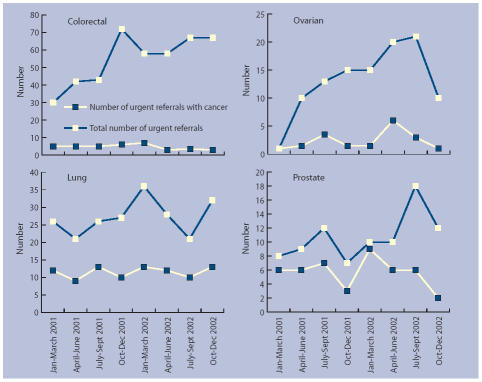
Method: Data regarding all urgent referrals and all cancer diagnoses were obtained from one hospital trust over a 2-year period. Data analysis was undertaken to determine, diagnostic yields and their association with sociodemographic factors, trends over time and fulfilment of the guidance.
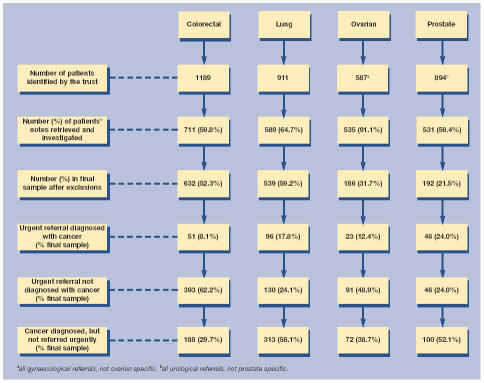
Results: The percentages of urgent referrals diagnosed with cancer were colorectal 11%, lung 42%, ovarian 20%, and prostate 50%. The percentages of patients with cancer referred urgently were colorectal 21%, lung 23%, ovarian 24%, and prostate 32%. Patients who were urgently referred without cancer were younger than those with cancer for all but prostate. There were no significant differences by sex, marital status or ethnicity. For patients with cancer there were no differences for any sociodemographic factors in whether or not they were referred urgently.
Conclusions: The predictive power of the referral guidance as a marker for cancer is low, resulting in significant numbers of patients being urgently referred without cancer. A large majority of patients not diagnosed with cancer through the urgent referral route did fulfil the criteria for urgent referral, suggesting that with more widespread use of the guidance the diagnostic yields will be higher. This has implications for patients, on hospital diagnostic systems, and for patients presenting through other pathways.
Figures
References
-
- NHS Executive. The New NHS modern and dependable: a national framework for assessing performance. London: 1998.
-
- Department of Health. Referral guidelines for suspected cancer. London: Department of Health; 2000.
-
- Department of Health. The NHS cancer plan. London: Department of Health; 2000.
-
- National Institute for Health and Clinical Excellence. Referral guidelines for suspected cancer. Clinical guideline 27. London: National Institute for Health and Clinical Excellence; 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources