

Predictors of neurocognitive decline after carotid endarterectomy
- PMID: 16639318
- PMCID: PMC2562551
- DOI: 10.1227/01.NEU.0000209638.62401.7E
Predictors of neurocognitive decline after carotid endarterectomy
Expression of concern in
-
Editorial Expression of Concern.Neurosurgery. 2023 Aug 1;93(2):489. doi: 10.1227/neu.0000000000002565. Epub 2023 Jun 9. Neurosurgery. 2023. PMID: 37293834 No abstract available.
Abstract
Objective: Although the incidence of stroke after carotid endarterectomy (CEA) is low (1-3%), approximately 25% of patients experience subtle declines in postoperative neuropsychometric function. No studies have investigated the risk factors for this neurocognitive change. We sought to identify predictors of postoperative neurocognitive dysfunction.
Methods: We enrolled 186 CEA patients, with both symptomatic and asymptomatic stenosis, to undergo a battery of neuropsychometric tests preoperatively and on postoperative Days 1 and 30. Neurocognitive dysfunction was defined as a two standard deviation decline in performance compared with a similarly aged control group of lumbar laminectomy patients. Univariate logistic regression was performed for age, sex, obesity, smoking, symptomatology, diabetes mellitus, hypertension, hypercholesterolemia, use of statin medication, previous myocardial infarction, previous CEA, operative side, duration of surgery, duration of carotid cross-clamp, and weight-adjusted doses of midazolam and fentanyl. Variables achieving univariate P < 0.10 were included in a multivariate analysis. Data is presented as (odds ratio, 95% confidence interval, P-value).
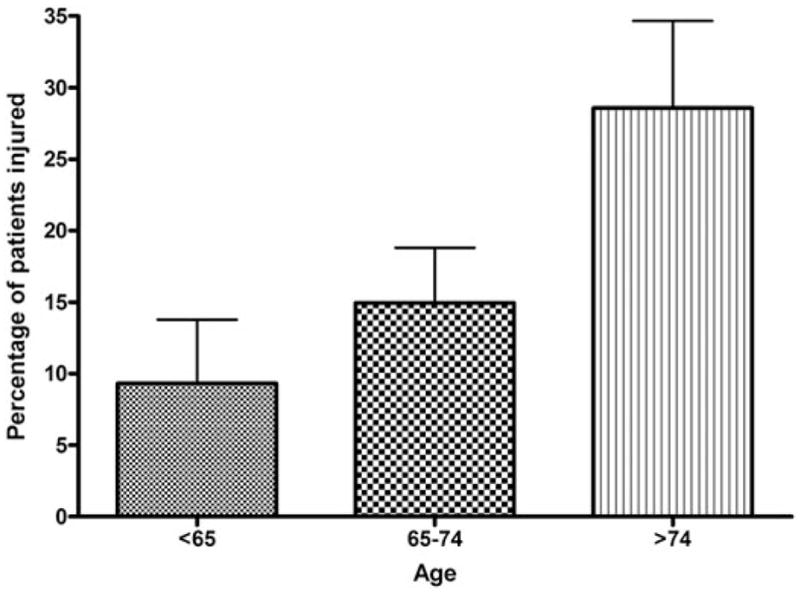
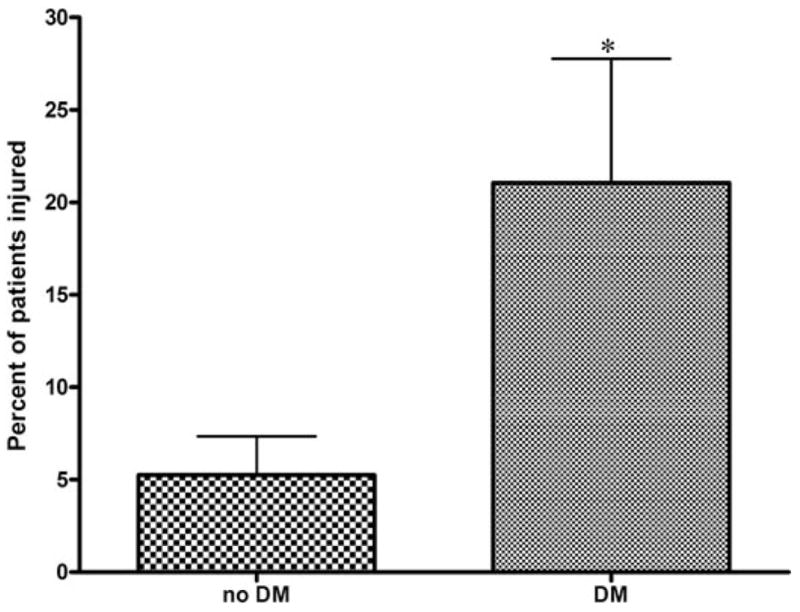
Results: Eighteen and 9% of CEA patients were injured on postoperative Days 1 and 30, respectively. Advanced age predicted neurocognitive dysfunction on Days 1 and 30 (1.93 per decade, 1.15-3.25, 0.01; and 2.57 per decade, 1.01-6.51, 0.049, respectively). Additionally, diabetes independently predicted injury on Day 30 (4.26, 1.15-15.79, 0.03).
Conclusions: Advanced age and diabetes predispose to neurocognitive dysfunction after CEA. These results are consistent with risk factors for neurocognitive dysfunction after coronary bypass and major stroke after CEA, supporting an underlying ischemic pathophysiology. Further work is necessary to determine the role these neurocognitive deficits may play in appropriately selecting patients for CEA.
Figures
References
-
- Barnett HJ. Carotid endarterectomy. Lancet. 2004;363:1486–1487. - PubMed
-
- Borowicz LM, Goldsborough MA, Selnes OA, McKhann GM. Neuropsychologic change after cardiac surgery: A critical review. J Cardiothorac Vasc Anesth. 1996;10:105–111. - PubMed
-
- Dodick DW, Meissner I, Meyer FB, Cloft HJ. Evaluation and management of asymptomatic carotid artery stenosis. Mayo Clin Proc. 2004;79:937–944. - PubMed
-
- Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995;273:1421–1428. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
