

A model of the natural history of screen-detected prostate cancer, and the effect of radical treatment on overall survival
- PMID: 16641912
- PMCID: PMC2361275
- DOI: 10.1038/sj.bjc.6603105
A model of the natural history of screen-detected prostate cancer, and the effect of radical treatment on overall survival
Abstract
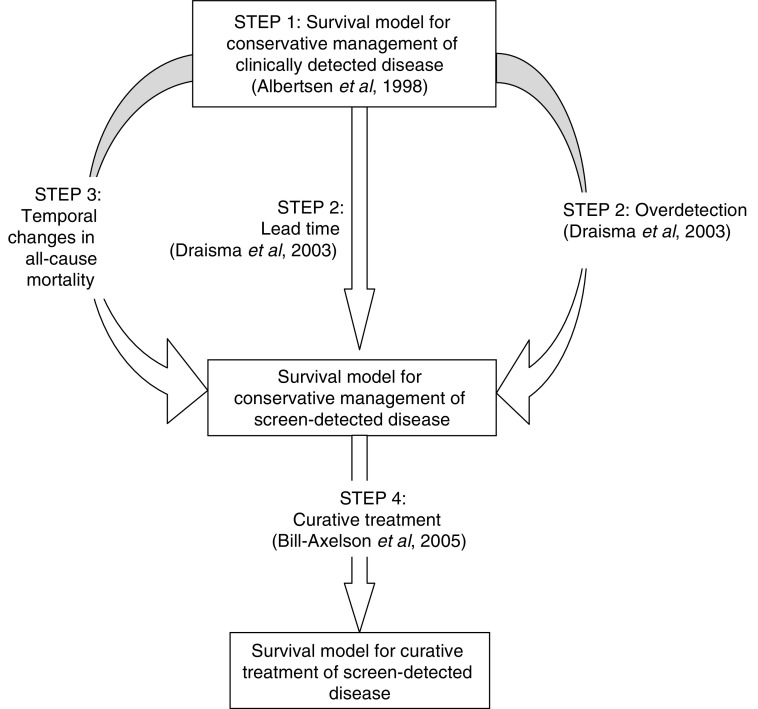
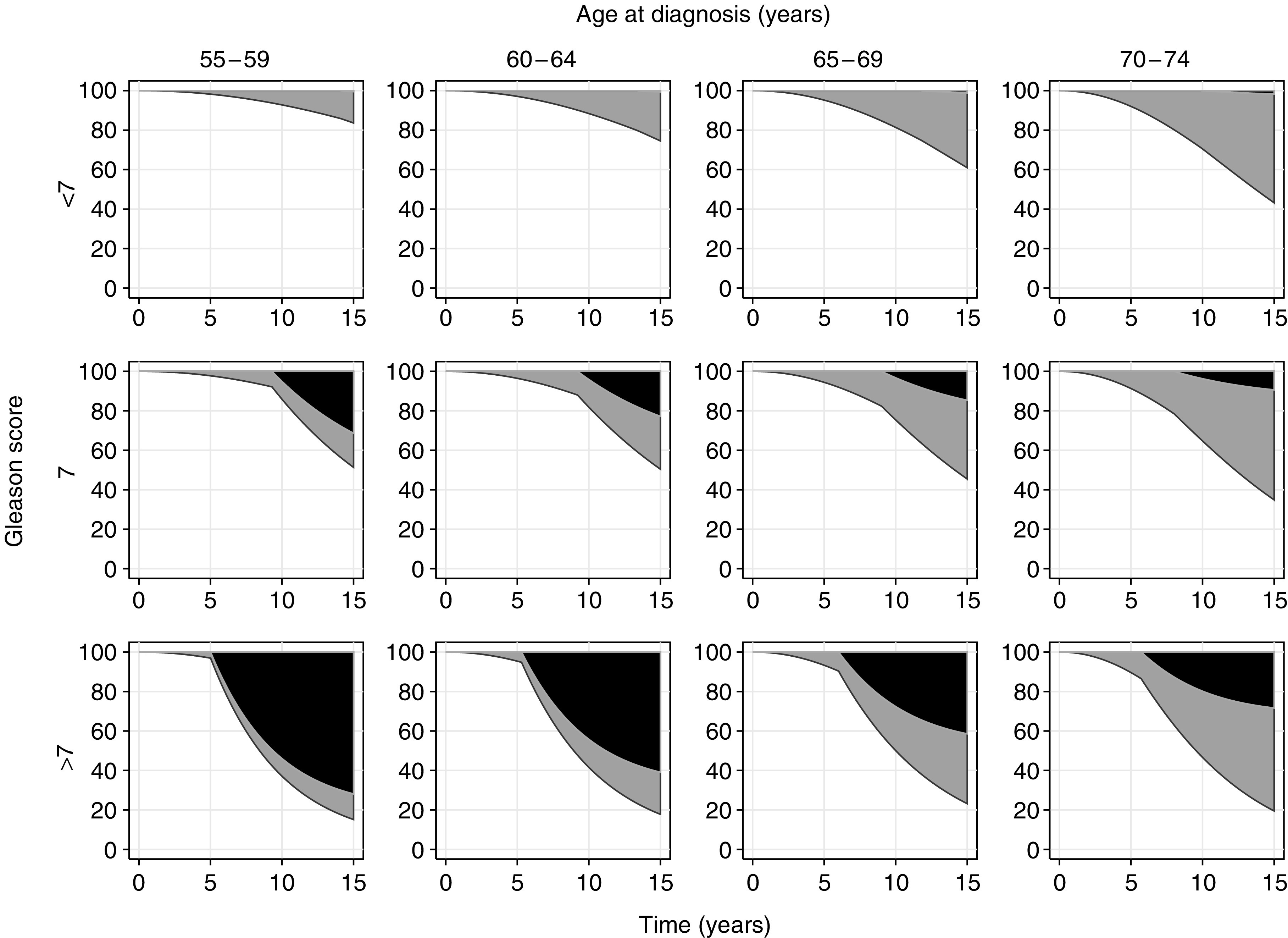
The lead time and over-detection associated with prostate-specific antigen (PSA) screening, and generational improvements in all-cause mortality, make prostate cancer outcome studies from the pre-PSA era difficult to interpret in a contemporary setting. We developed a competing-risks hazard model to estimate the natural history of screen-detected prostate cancer, and the impact of radical treatment on overall survival. The model of hazard of mortality was fitted to clinical outcome data from the pre-PSA era, and the effects of screening, generational mortality improvements and radical treatment were incorporated. Sensitivities to the choice of baseline data and values of key parameters were assessed. Lead-time estimates in men diagnosed aged 55-59 years were 14.1, 9.3 and 5.0 years for men with Gleason scores <7, 7 and >7, respectively, assuming biennial screening with 100% attendance. Central estimates of 15-year prostate cancer mortality for conservative management of screen-detected prostate cancer ranged from 0 to 2% for Gleason scores <7, 9 to 31% for Gleason score 7 and 28-72% for Gleason scores >7. For men aged 55-59 years at diagnosis, the predicted absolute 15-year survival benefit from curative treatment was 0, 12 and 26% for men with Gleason scores <7, 7 and >7, respectively. Estimates of the survival benefit of radical treatment were relatively insensitive to values of key parameters. The case for curative treatment, rather than conservative management, of screen-detected localised prostate cancer is strongest in men with high-grade disease. This conclusion contrasts with current patterns of care.
Figures
Comment in
-
A model of the natural history of screen-detected prostate cancer.Br J Cancer. 2006 Oct 23;95(8):1122-3. doi: 10.1038/sj.bjc.6603368. Epub 2006 Sep 26. Br J Cancer. 2006. PMID: 17003784 Free PMC article. No abstract available.
References
-
- Albertsen P, Gleason D, Barry M (1998) Competing risk analysis of men aged 55 to 74 years at diagnosis managed conservatively for clinically localized prostate cancer. JAMA 280: 975–980 - PubMed
-
- Albertsen PC, Hanley JA, Fine J (2005) 20-year outcomes following conservative management of clinically localized prostate cancer. JAMA 293: 2095–2101 - PubMed
-
- Anderson P, Abildstrom S, Rosthoj S (2002) Competing risks as a multi-state model. Stat Methods Med Res 11: 203–215 - PubMed
-
- Barry MJ, Albertsen PC, Bagshaw MA, Blute ML, Cox R, Middleton RG, Gleason DF, Zincke H, Bergstralh EJ, Jacobsen SJ (2001) Outcomes for men with clinically nonmetastatic prostate carcinoma managed with radical prostactectomy, external beam radiotherapy, or expectant management: a retrospective analysis. Cancer 91: 2302–2314 - PubMed
-
- Bill-Axelson A, Holmberg L, Ruutu M, Haggman M, Andersson SO, Bratell S, Spangberg A, Busch C, Nordling S, Garmo H, Palmgren J, Adami HO, Norlen BJ, Johansson JE (2005) Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 352: 1977–1984 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
