

Migraine care among different ethnicities: do disparities exist?
- PMID: 16643578
- PMCID: PMC2443411
- DOI: 10.1111/j.1526-4610.2006.00453.x
Migraine care among different ethnicities: do disparities exist?
Abstract
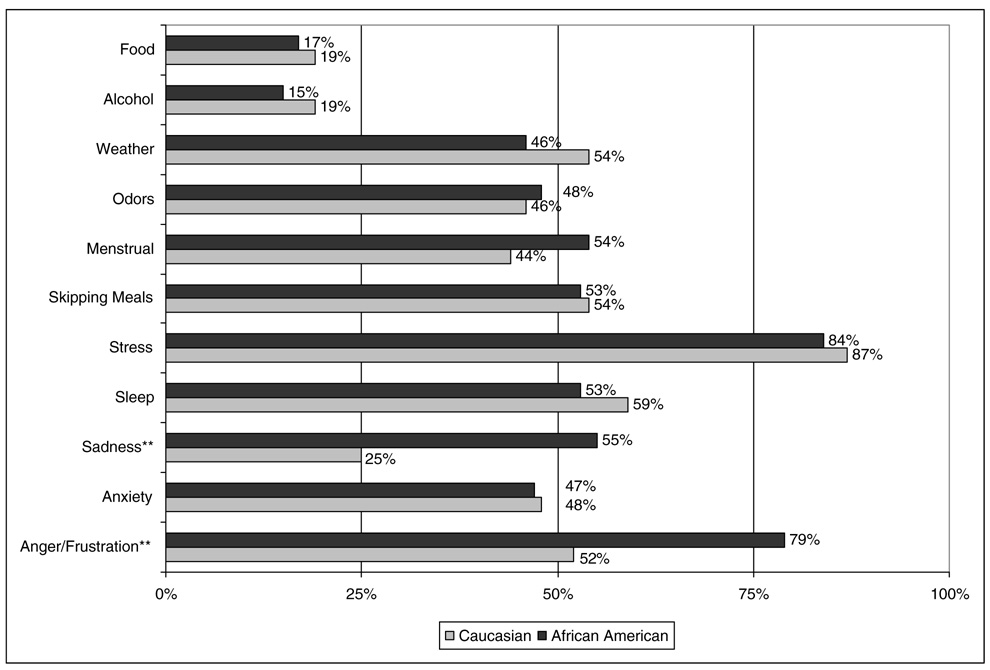
Objective: Evaluate whether, in a primary care setting, Caucasians (C) and African Americans (AA) with moderately to severely disabling migraines differed in regards to: utilizing the health-care system for migraine care, migraine diagnosis and treatment, level of mistrust in the health-care system, perceived communication with their physician, and perceived migraine triggers.
Background: Research has documented ethnic disparities in pain management. However, almost no research has been published concerning potential disparities in utilization, diagnosis, and/or treatment of migraine. It is also important to consider whether ethnic differences exist for trust and communication between patients and physicians, as these are essential when diagnosing and treating migraine.
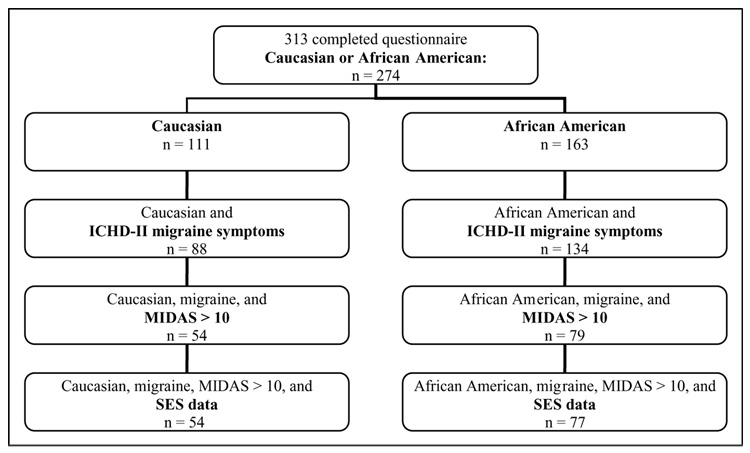
Methods: Adult patients with headache (n = 313) were recruited from primary care waiting rooms. Of these, 131 (AA = 77; C = 54) had migraine, moderate to severe headache-related disability, and provided socioeconomic status (SES) data. Participants completed measures of migraine disability (MIDAS), migraine health-care utilization, diagnosis and treatment history, mistrust of the medical community, patient-physician communication (PPC), and migraine triggers. Analysis of covariance (controlling for SES and recruitment site), chi-square, and Pearson product moment correlations were conducted.
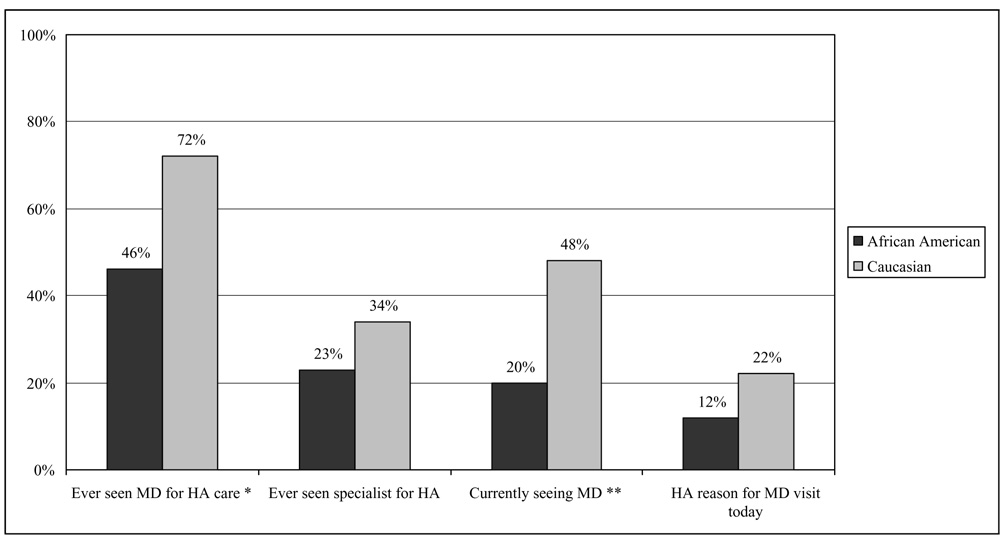
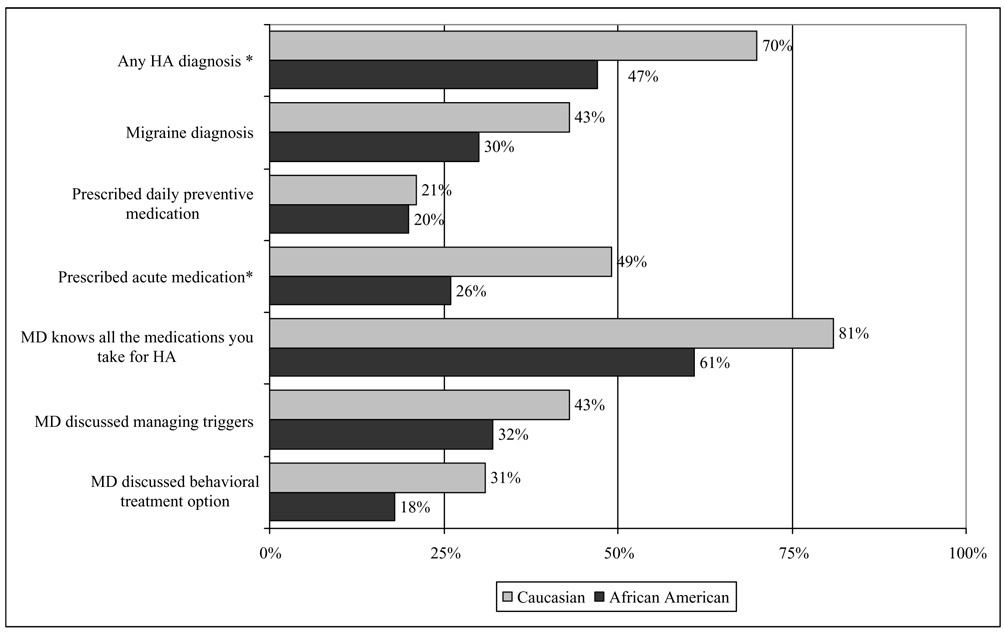
Results: African Americans were less likely to utilize the health-care setting for migraine treatment (AA = 46% vs. C = 72%, P < .001), to have been given a headache diagnosis (AA = 47% vs. C = 70%, P < .001), and to have been prescribed acute migraine medication (AA = 14% vs. C = 37%, P < .001). Migraine diagnosis was low for both groups, and <15% of all participants had been prescribed a migraine-specific medication or a migraine preventive medication despite suffering moderate to severe levels of migraine disability. African Americans had less trust in the medical community (P < .001, eta2 = 0.26) and less positive PPC (P < .001, eta2 = 0.11). Also, the lower the trust and communication, the less likely they were to have ever seen (or currently be seeing) a doctor for migraine care or to have been prescribed medication.
Conclusions: Migraine utilization, diagnosis, and treatment were low for both groups. However, this was especially true for African Americans, who also reported lower levels of trust and communication with doctors relative to Caucasians. The findings highlight the need for improved physician and patient education about migraine diagnosis and treatment, the importance of cultural variation in pain presentation, and the importance of communication when diagnosing and treating migraine.
Conflict of interest statement
Figures
References
-
- Smedley B, Stith A, Nelson A. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academies Press; 2002. - PubMed
-
- The Morehouse Medical Treatment and Effectiveness Center. Racial & Ethnic Differences in Access to Medical Care: A Synthesis of the Literature. Menlo Park, CA: The Henry J. Kaiser Family Foundation; 2000.
-
- Gornick ME, Eggers PW, Reilly TW, Mentnech RM, Fitterman LK, Kucken LE, et al. Effects of race and income on mortality and use of services among Medicare beneficiaries. N Engl J Med. 1996;335:791–799. - PubMed
-
- Ferguson JA, Tierney WM, Westmoreland GR, et al. Examination of racial differences in management of cardiovascular disease. J Am Coll Cardiol. 1997;30:1707–1713. - PubMed
-
- Moore RD, Stanton D, Gopalan R, Chaisson RE. Racial differences in the use of drug therapy for HIV disease in an urban community. N Engl J Med. 1994;330:763–768. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
