

Primary histologic diagnosis using automated whole slide imaging: a validation study
- PMID: 16643664
- PMCID: PMC1525169
- DOI: 10.1186/1472-6890-6-4
Primary histologic diagnosis using automated whole slide imaging: a validation study
Abstract
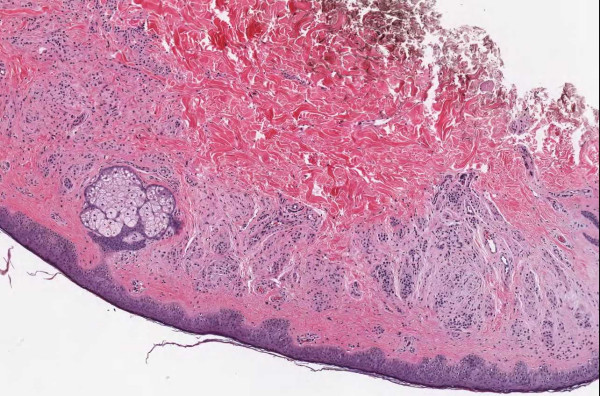
Background: Only prototypes 5 years ago, high-speed, automated whole slide imaging (WSI) systems (also called digital slide systems, virtual microscopes or wide field imagers) are becoming increasingly capable and robust. Modern devices can capture a slide in 5 minutes at spatial sampling periods of less than 0.5 micron/pixel. The capacity to rapidly digitize large numbers of slides should eventually have a profound, positive impact on pathology. It is important, however, that pathologists validate these systems during development, not only to identify their limitations but to guide their evolution.
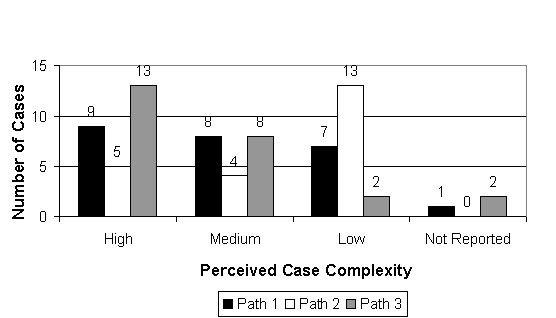
Methods: Three pathologists fully signed out 25 cases representing 31 parts. The laboratory information system was used to simulate real-world sign-out conditions including entering a full diagnostic field and comment (when appropriate) and ordering special stains and recuts. For each case, discrepancies between diagnoses were documented by committee and a "consensus" report was formed and then compared with the microscope-based, sign-out report from the clinical archive.
Results: In 17 of 25 cases there were no discrepancies between the individual study pathologist reports. In 8 of the remaining cases, there were 12 discrepancies, including 3 in which image quality could be at least partially implicated. When the WSI consensus diagnoses were compared with the original sign-out diagnoses, no significant discrepancies were found. Full text of the pathologist reports, the WSI consensus diagnoses, and the original sign-out diagnoses are available as an attachment to this publication.
Conclusion: The results indicated that the image information contained in current whole slide images is sufficient for pathologists to make reliable diagnostic decisions and compose complex diagnostic reports. This is a very positive result; however, this does not mean that WSI is as good as a microscope. Virtually every slide had focal areas in which image quality (focus and dynamic range) was less than perfect. In some cases, there was evidence of over-compression and regions made "soft" by less than perfect focus. We expect systems will continue to get better, image quality and speed will continue to improve, but that further validation studies will be needed to guide development of this promising technology.
Figures

























References
-
- Black CA, Lavoie HA, Millette CF. Teaching medical histology at the University of South Carolina School of Medicine: transition to virtual slides and virtual microscopes. Anatomical Record Part B, The New Anatomist. 2003;275:196–206. - PubMed
-
- Gagnon M, Inhorn S, Hancock J, Keller B, Carpenter D, Merlin T, Hearn T, Thompson P, Whalen R. Comparison of cytology proficiency testing: glass slides vs. virtual slides. Acta Cytol. 2004;48:788–794. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
