

Peripheral T-cell lymphoma-unspecified (PTCL-U) presenting with hypereosinophilic syndrome and pleural effusions
- PMID: 16646567
- PMCID: PMC3891066
- DOI: 10.3904/kjim.2006.21.1.57
Peripheral T-cell lymphoma-unspecified (PTCL-U) presenting with hypereosinophilic syndrome and pleural effusions
Abstract
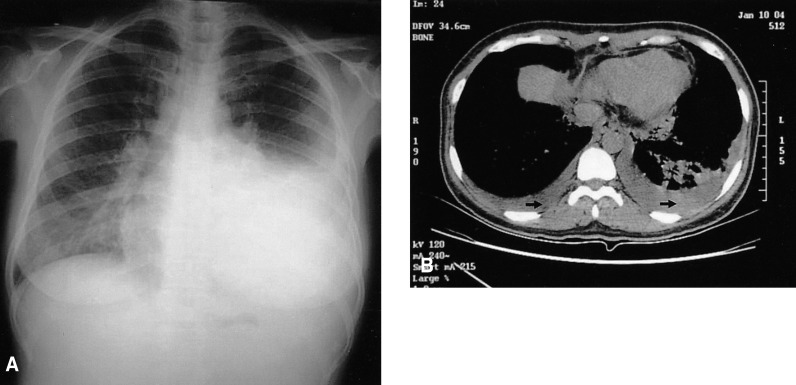
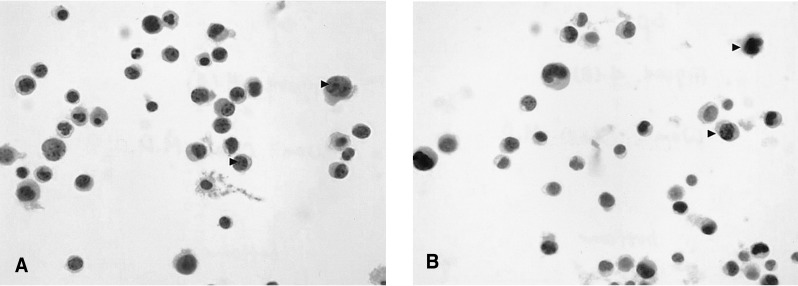
Hypereosinophilic syndrome (HES) is a clinical disorder characterized by persistent eosinophilia and systemic involvement, in which a specific causative factor for the eosinophilia cannot be verified during a certain period of time. There have been only a few reported cases of this syndrome associated with malignant lymphoma. We report a case of peripheral T-cell lymphoma-unspecified with hypereosinophilic syndrome. The patient was a 42-year-old woman with an uncontrolled fever and a sore throat. Eosinophilia was observed on the peripheral blood smear. We confirmed the diagnosis by bone marrow and liver biopsies:. A bone marrow aspiration demonstrated markedly increased eosinophils (24.8%), and a liver biopsy demonstrated infiltration by scattered eosinophils and atypical lymphoid cells, which were confirmed to be T-cell lymphoma cells. This case was a distinctive presentation of peripheral T-cell lymphoma with hypereosinophilic syndrome, probably due to a paraneoplastic condition.
Figures





References
-
- Hardy WR, Ancerson R. The hypereosinophilic syndrome. Ann Intern Med. 1968;68:1220–1229. - PubMed
-
- Chusid MJ, Dale DC, West BC, Wolff SM. The hypereosinophilic syndrome: analysis of 14 cases with review of the literature. Medicine. 1975;54:1–27. - PubMed
-
- Fauci AS, Harley JB, Robert WC, Ferrans VJ, Gralnick HR, Bjornson BH. The idiopathic hypereosinophilic syndrome: clinical, pathophysiologic, and therapeutic consideration. Ann Intern Med. 1982;97:78–92. - PubMed
-
- Berki T, David M, Bone B, Losonczy H, Vass J, Nemeth P. New diagnostic tool for differentiation of idiopathic hypereosinophilic syndrome and secondary eosinophilic states. Pathol Oncol Res. 2001;7:292–297. - PubMed
-
- Bunc M, Remskar A, Brucan A. The idiopathic hypereosinophilic syndrome. Eur J Emerg Med. 2001;8:325–330. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical