

Efficacy and safety of non-invasive ventilation in the treatment of acute cardiogenic pulmonary edema--a systematic review and meta-analysis
- PMID: 16646987
- PMCID: PMC1550884
- DOI: 10.1186/cc4905
Efficacy and safety of non-invasive ventilation in the treatment of acute cardiogenic pulmonary edema--a systematic review and meta-analysis
Abstract
Introduction: Continuous positive airway pressure ventilation (CPAP) and non-invasive positive pressure ventilation (NPPV) are accepted treatments in acute cardiogenic pulmonary edema (ACPE). However, it remains unclear whether NPPV is better than CPAP in reducing the need for endotracheal intubation (NETI) rates, mortality and other adverse events. Our aim was to review the evidence about the efficacy and safety of these two methods in ACPE management.
Methods: We conducted a systematic review and meta-analysis of randomized controlled trials on the effect of CPAP and/or NIPV in the treatment of ACPE, considering the outcomes NETI, mortality and incidence of acute myocardial infarction (AMI). We searched six electronic databases up to May 2005 without language restrictions, reviewed references of relevant articles, hand searched conference proceedings and contacted experts.
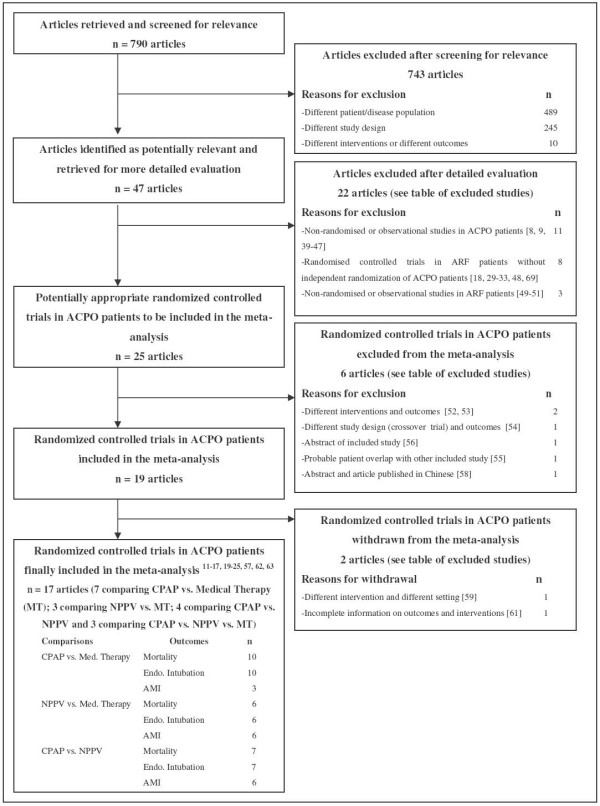
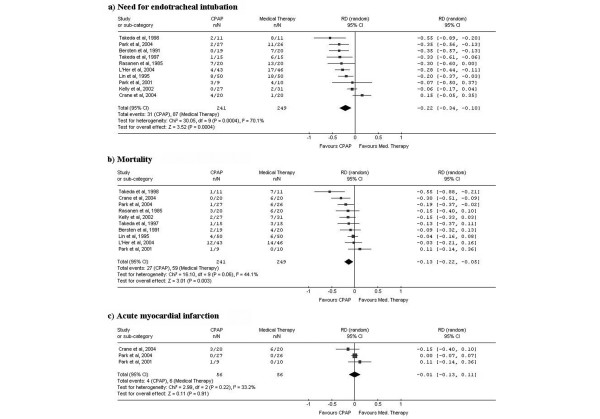
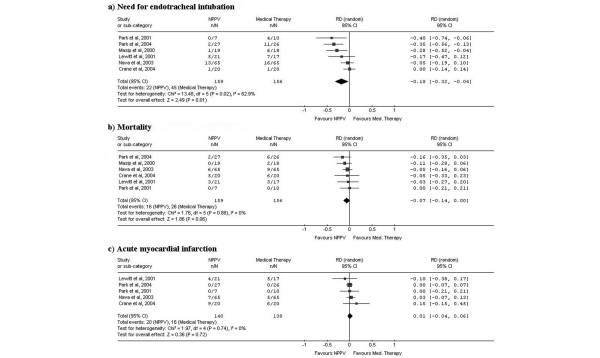
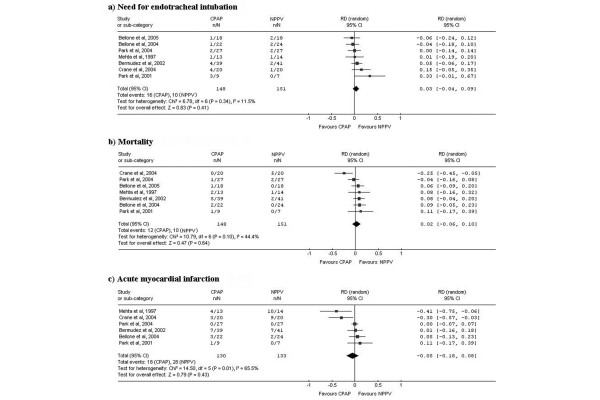
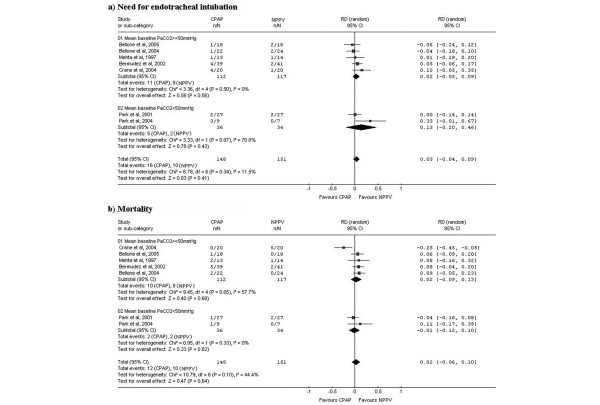
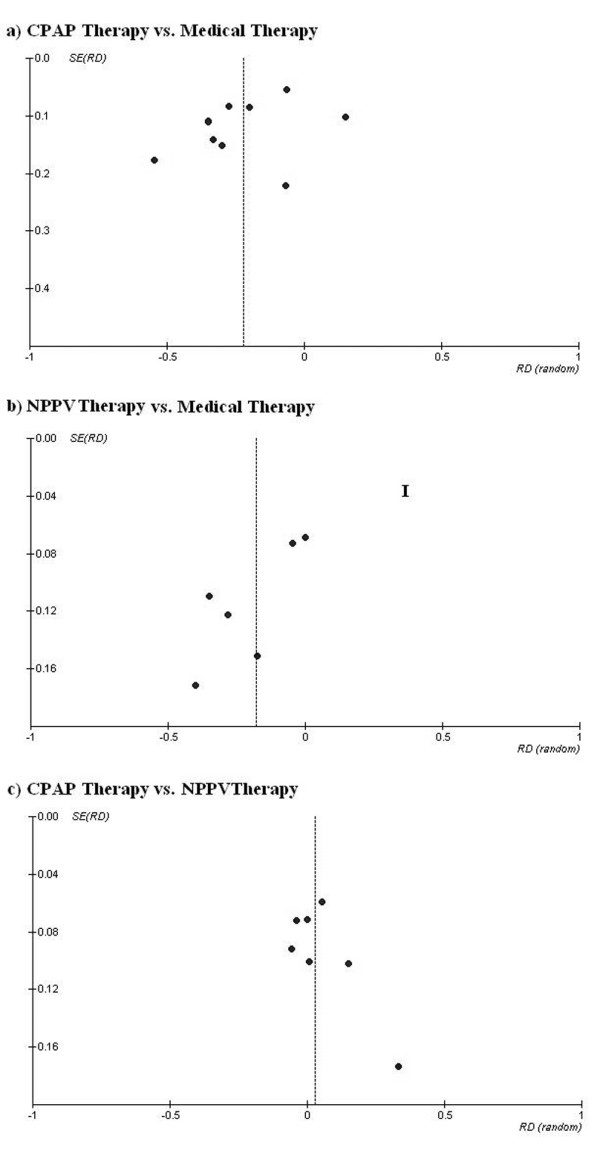
Results: Of 790 articles identified, 17 were included. In a pooled analysis, 10 studies of CPAP compared to standard medical therapy (SMT) showed a significant 22% absolute risk reduction (ARR) in NETI (95% confidence interval (CI), -34% to -10%) and 13% in mortality (95%CI, -22% to -5%). Six studies of NPPV compared to SMT showed an 18% ARR in NETI (95%CI, -32% to -4%) and 7% in mortality (95%CI, -14% to 0%). Seven studies of NPPV compared to CPAP showed a non-significant 3% ARR in NETI (95%CI, -4% to 9%) and 2% in mortality (95%CI, -6% to 10%). None of these methods increased AMI risk. In a subgroup analysis, NPPV did not lead to better outcomes than CPAP in studies including more hypercapnic patients.
Conclusion: Robust evidence now supports the use of CPAP and NPPV in ACPE. Both techniques decrease NETI and mortality compared to SMT and none shows increased AMI risk. CPAP should be considered a first line intervention as NPPV did not show a better efficacy, even in patients with more severe conditions, and CPAP is cheaper and easier to implement in clinical practice.
Figures
References
-
- American Heart Association . 2004 Heart and Stroke statistical update. Dallas, Texas: American Heart Association; 2004.
-
- Fonarow G, ADHERE scientific advisory committee The acute decompensated heart failure national registry (ADHERE): opportunities to improve care of patients hospitalized with acute decompensated heart failure. Rev Cardiovasc Med. 2003;4(Suppl 7):S21–30. - PubMed
-
- Fedullo AJ, Swinburne AJ, Wahl GW, Bixby K. Acute cardiogenic pulmonary edema treated with mechanical ventilation. Factors determining in-hospital mortality. Chest. 1991;99:1220–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
