

Cytokine-mediated deployment of SDF-1 induces revascularization through recruitment of CXCR4+ hemangiocytes
- PMID: 16648859
- PMCID: PMC2754288
- DOI: 10.1038/nm1400
Cytokine-mediated deployment of SDF-1 induces revascularization through recruitment of CXCR4+ hemangiocytes
Erratum in
- Nat Med. 2006 Aug;12(8):978
Abstract
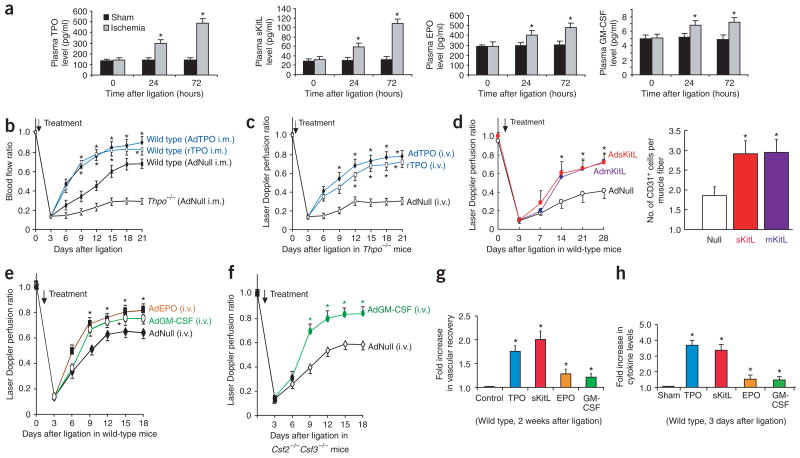
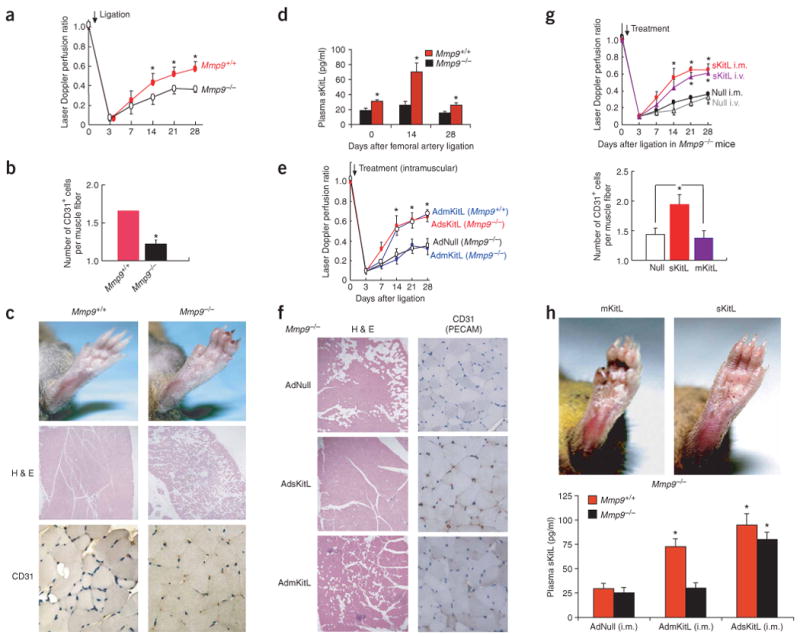
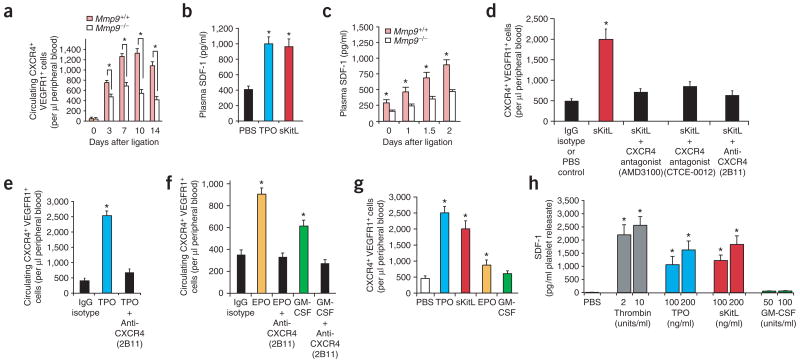
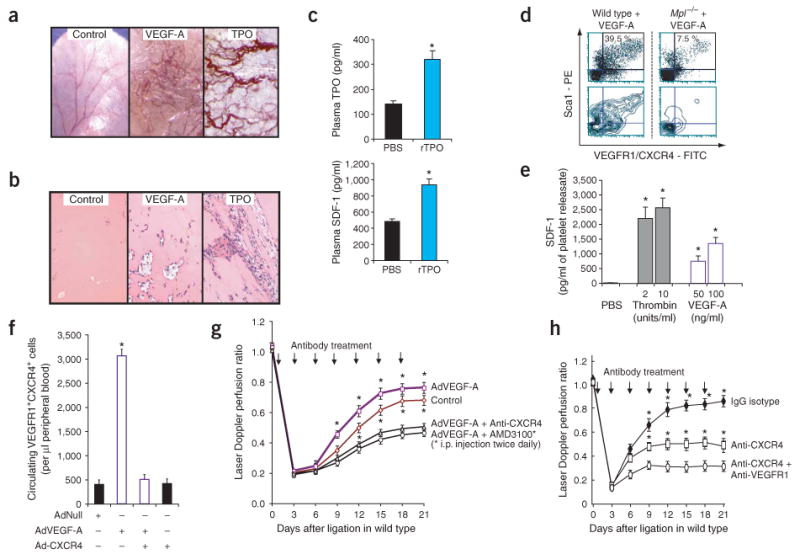
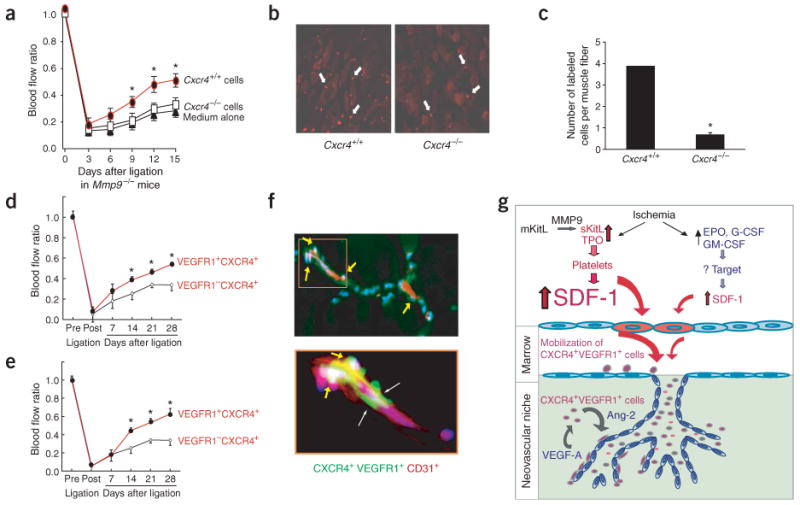
The mechanisms through which hematopoietic cytokines accelerate revascularization are unknown. Here, we show that the magnitude of cytokine-mediated release of SDF-1 from platelets and the recruitment of nonendothelial CXCR4+ VEGFR1+ hematopoietic progenitors, 'hemangiocytes,' constitute the major determinant of revascularization. Soluble Kit-ligand (sKitL), thrombopoietin (TPO, encoded by Thpo) and, to a lesser extent, erythropoietin (EPO) and granulocyte-macrophage colony-stimulating factor (GM-CSF) induced the release of SDF-1 from platelets, enhancing neovascularization through mobilization of CXCR4+ VEGFR1+ hemangiocytes. Although revascularization of ischemic hindlimbs was partially diminished in mice deficient in both GM-CSF and G-CSF (Csf2-/- Csf3-/-), profound impairment in neovascularization was detected in sKitL-deficient Mmp9-/- as well as thrombocytopenic Thpo-/- and TPO receptor-deficient (Mpl-/-) mice. SDF-1-mediated mobilization and incorporation of hemangiocytes into ischemic limbs were impaired in Thpo-/-, Mpl-/- and Mmp9-/- mice. Transplantation of CXCR4+ VEGFR1+ hemangiocytes into Mmp9-/- mice restored revascularization, whereas inhibition of CXCR4 abrogated cytokine- and VEGF-A-mediated mobilization of CXCR4+ VEGFR1+ cells and suppressed angiogenesis. In conclusion, hematopoietic cytokines, through graded deployment of SDF-1 from platelets, support mobilization and recruitment of CXCR4+ VEGFR1+ hemangiocytes, whereas VEGFR1 is essential for their angiogenic competency for augmenting revascularization. Delivery of SDF-1 may be effective in restoring angiogenesis in individuals with vasculopathies.
Conflict of interest statement
Figures

References
-
- Rafii S, Lyden D. Therapeutic stem and progenitor cell transplantation for organ vascularization and regeneration. Nat Med. 2003;9:702–712. - PubMed
-
- Takakura N, et al. A role for hematopoietic stem cells in promoting angiogenesis. Cell. 2000;102:199–209. - PubMed
-
- Aicher A, et al. Essential role of endothelial nitric oxide synthase for mobilization of stem and progenitor cells. Nat Med. 2003;9:1370–1376. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
