

The atypical pneumonias: clinical diagnosis and importance
- PMID: 16669925
- PMCID: PMC7128183
- DOI: 10.1111/j.1469-0691.2006.01393.x
The atypical pneumonias: clinical diagnosis and importance
Abstract
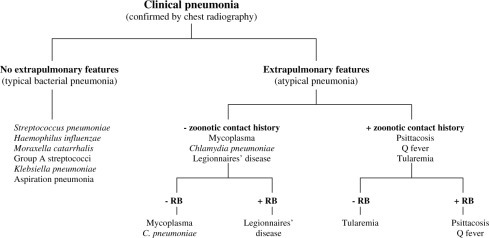
The most common atypical pneumonias are caused by three zoonotic pathogens, Chlamydia psittaci (psittacosis), Francisella tularensis (tularemia), and Coxiella burnetii (Q fever), and three nonzoonotic pathogens, Chlamydia pneumoniae, Mycoplasma pneumoniae, and Legionella. These atypical agents, unlike the typical pathogens, often cause extrapulmonary manifestations. Atypical CAPs are systemic infectious diseases with a pulmonary component and may be differentiated clinically from typical CAPs by the pattern of extrapulmonary organ involvement which is characteristic for each atypical CAP. Zoonotic pneumonias may be eliminated from diagnostic consideration with a negative contact history. The commonest clinical problem is to differentiate legionnaire's disease from typical CAP as well as from C. pneumoniae or M. pneumonia infection. Legionella is the most important atypical pathogen in terms of severity. It may be clinically differentiated from typical CAP and other atypical pathogens by the use of a weighted point system of syndromic diagnosis based on the characteristic pattern of extrapulmonary features. Because legionnaire's disease often presents as severe CAP, a presumptive diagnosis of Legionella should prompt specific testing and empirical anti-Legionella therapy such as the Winthrop-University Hospital Infectious Disease Division's weighted point score system. Most atypical pathogens are difficult or dangerous to isolate and a definitive laboratory diagnosis is usually based on indirect, i.e., direct flourescent antibody (DFA), indirect flourescent antibody (IFA). Atypical CAP is virtually always monomicrobial; increased IFA IgG tests indicate past exposure and not concurrent infection. Anti-Legionella antibiotics include macrolides, doxycycline, rifampin, quinolones, and telithromycin. The drugs with the highest level of anti-Legionella activity are quinolones and telithromycin. Therapy is usually continued for 2 weeks if potent anti-Legionella drugs are used. In adults, M. pneumoniae and C. pneumoniae may exacerbate or cause asthma. The importance of the atypical pneumonias is not related to their frequency (approximately 15% of CAPs), but to difficulties in their diagnosis, and their nonresponsiveness to beta-lactam therapy. Because of the potential role of C. pneumoniae in coronary artery disease and multiple sclerosis (MS), and the role of M. pneumoniae and C. pneumoniae in causing or exacerbating asthma, atypical CAPs also have public health importance.
Figures
References
-
- Murray HW, Tuazon C. Atypical pneumonias. Med Clin North Am. 1980;64:507–527. - PubMed
-
- Martin RE, Bates JH. Atypical pneumonia. Infect Dis Clin North Am. 1991;5:585–601. - PubMed
-
- Blasi F. Atypical pathogens and respiratory tract infections. Eur Respir J. 2004;24:171–181. - PubMed
-
- Marrie TJ, editor. Community‐Acquired Pneumonia. Kluwer Academic; New York: 2001.
-
- Karetzky M, Cunha BA, Brandstetter RD. The Pneumonias. Springer‐Verlag; New York: 1993.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
