

Bronchial hyperresponsiveness and the development of asthma and COPD in asymptomatic individuals: SAPALDIA cohort study
- PMID: 16670173
- PMCID: PMC2104688
- DOI: 10.1136/thx.2005.052241
Bronchial hyperresponsiveness and the development of asthma and COPD in asymptomatic individuals: SAPALDIA cohort study
Abstract
Background: Bronchial hyperresponsiveness (BHR) is a common feature of asthma. However, BHR is also present in asymptomatic individuals and its clinical and prognostic significance is unclear. We hypothesised that BHR might play a role in the development of chronic obstructive pulmonary disease (COPD) as well as asthma.
Methods: In 1991 respiratory symptoms and BHR to methacholine were evaluated in 7126 of the 9651 participants in the SAPALDIA cohort study. Eleven years later 5825 of these participants were re-evaluated, of whom 4852 performed spirometric tests. COPD was defined as an FEV1/FVC ratio of <0.70.
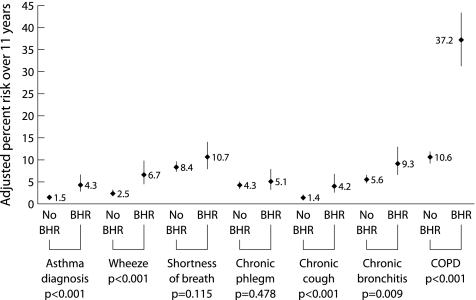
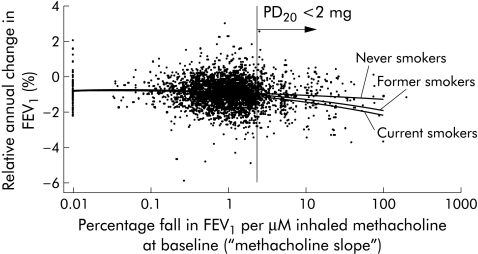
Results: In 1991 17% of participants had BHR, of whom 51% were asymptomatic. Eleven years later the prevalence of asthma, wheeze, and shortness of breath in formerly asymptomatic subjects with or without BHR was, respectively, 5.7% v 2.0%, 8.3% v 3.4%, and 19.1% v 11.9% (all p<0.001). Similar differences were observed for chronic cough (5.9% v 2.3%; p = 0.002) and COPD (37.9% v 14.3%; p<0.001). BHR conferred an adjusted odds ratio (OR) of 2.9 (95% CI 1.8 to 4.5) for wheezing at follow up among asymptomatic participants. The adjusted OR for COPD was 4.5 (95% CI 3.3 to 6.0). Silent BHR was associated with a significantly accelerated decline in FEV1 by 12 (5-18), 11 (5-16), and 4 (2-8) ml/year in current smokers, former smokers and never smokers, respectively, at SAPALDIA 2.
Conclusions: BHR is a risk factor for an accelerated decline in FEV1 and the development of asthma and COPD, irrespective of atopic status. Current smokers with BHR have a particularly high loss of FEV1.
Conflict of interest statement
Competing interests: none declared.
References
-
- Magnussen H, Richter K, Taube C. Are chronic obstructive pulmonary disease (COPD) and asthma different diseases? Clin Exp Allergy 199828(Suppl 5)187–94 2035. - PubMed