

T cell control in autoimmune bullous skin disorders
- PMID: 16670756
- PMCID: PMC1451217
- DOI: 10.1172/JCI28547
T cell control in autoimmune bullous skin disorders
Abstract
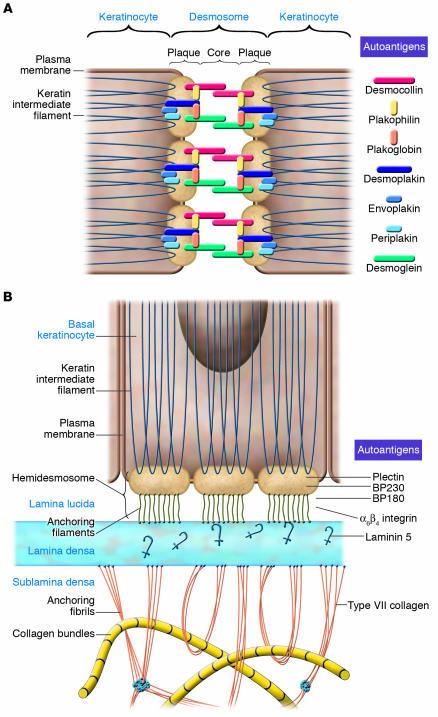
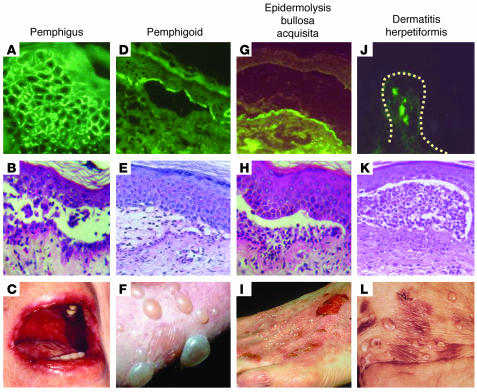
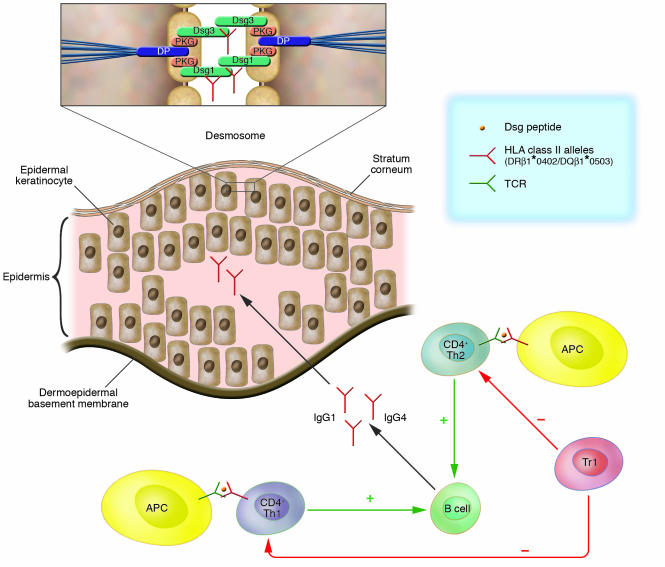
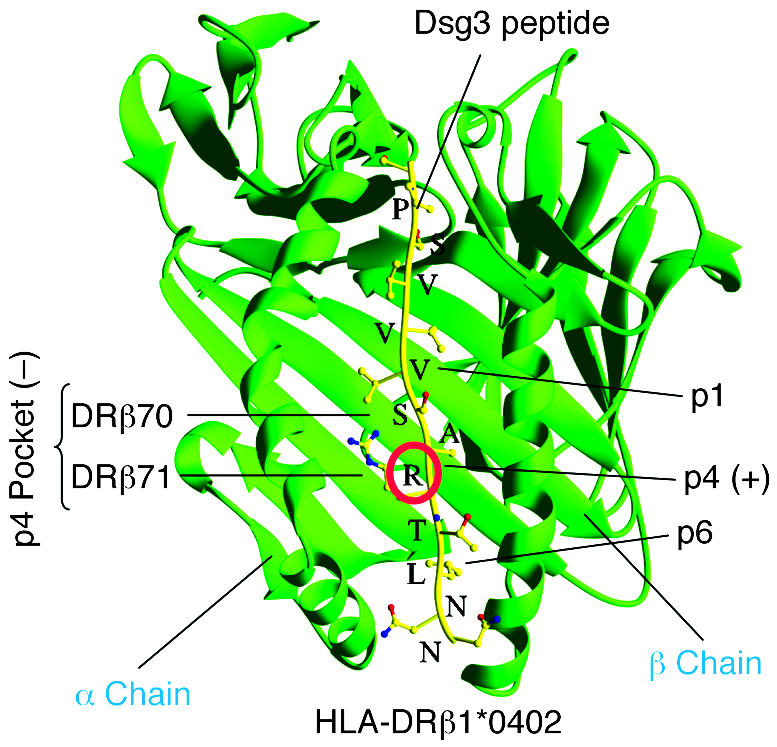
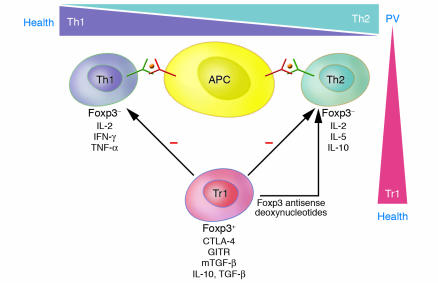
Autoimmune bullous disorders are a group of severe skin diseases characterized clinically by blisters and erosions of skin and/or mucous membranes. A hallmark of these disorders is the presence of IgG and occasionally IgA autoantibodies that target distinct adhesion structures of the epidermis, dermoepidermal basement membrane, and anchoring fibrils of the dermis. This Review focuses on the potential role of autoreactive T cells in the pathogenesis of these disorders. Pemphigus vulgaris (PV) and bullous pemphigoid (BP) are the best-characterized bullous disorders with regard to pathogenesis and T cell involvement. Activation of autoreactive T cells in PV and BP is restricted by distinct HLA class II alleles that are prevalent in individuals with these disorders. Autoreactive T cells are not only present in patients but can also be detected in healthy individuals. Recently, a subset of autoreactive T cells with remarkable regulatory function was identified in healthy individuals and to a much lesser extent in patients with PV, suggesting that the occurrence of autoimmune bullous disorders may be linked to a dysfunction of Tregs.
Figures
References
-
- Beutner E.H., Jordon R.E., Chorzelski T.P. The immunopathology of pemphigus and bullous pemphigoid. J. Invest. Dermatol. 1968;51:63–80. - PubMed
-
- Yancey K.B., Egan C.A. Pemphigoid: clinical, histologic, immunopathologic, and therapeutic considerations. JAMA. 2000;284:350–356. - PubMed
-
- Hertl M. Humoral and cellular autoimmunity in autoimmune bullous skin disorders. Int. Arch. Allergy Immunol. 2000;122:91–100. - PubMed
-
- Borradori L., Sonnenberg A. Hemidesmosomes: roles in adhesion, signaling and human diseases. Curr. Opin. Cell Biol. 1996;8:647–656. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
