

Prophylactic human papillomavirus vaccines
- PMID: 16670757
- PMCID: PMC1451224
- DOI: 10.1172/JCI28607
Prophylactic human papillomavirus vaccines
Abstract
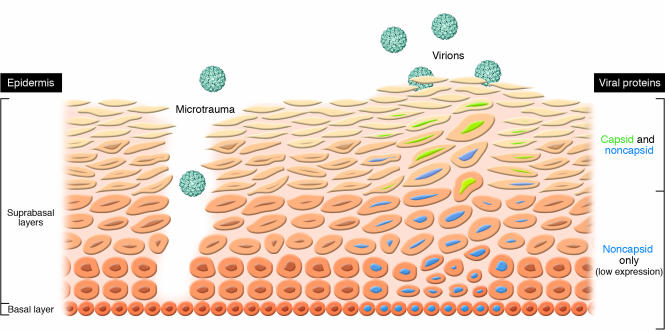
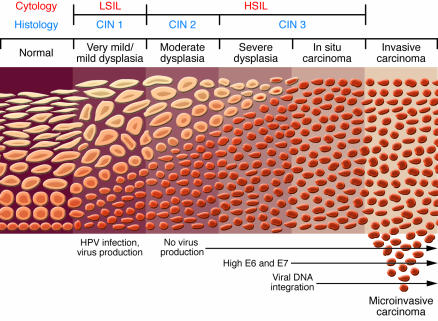
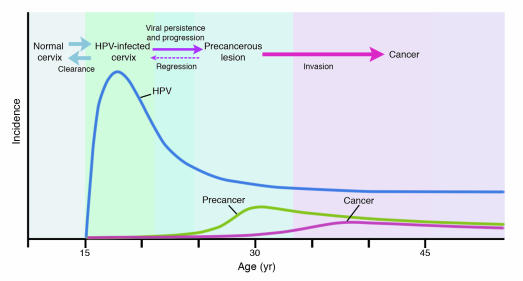
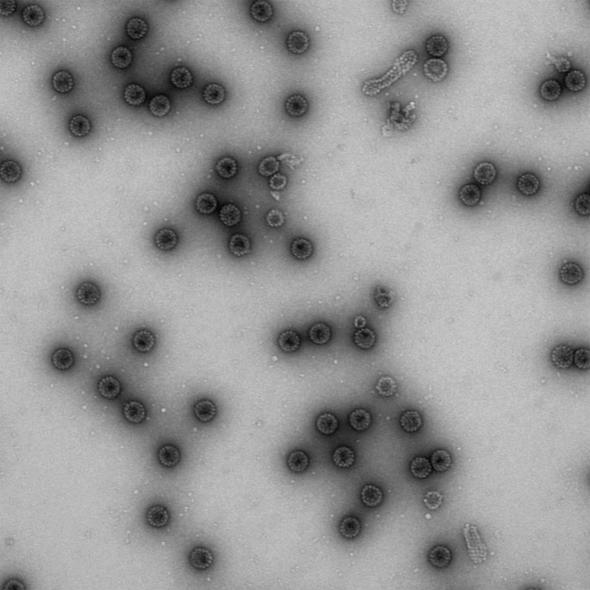
Human papillomavirus (HPV) infection causes virtually all cases of cervical cancer, the second most common cause of death from cancer among women worldwide. This Review examines prophylactic HPV subunit vaccines based on the ability of the viral L1 capsid protein to form virus-like particles (VLPs) that induce high levels of neutralizing antibodies. Following preclinical research by laboratories in the nonprofit sector, Merck and GlaxoSmithKline are developing commercial versions of the vaccine. Both vaccines target HPV16 and HPV18, which account for approximately 70% of cervical cancer. The Merck vaccine also targets HPV6 and HPV11, which account for approximately 90% of external genital warts. The vaccines have an excellent safety profile, are highly immunogenic, and have conferred complete type-specific protection against persistent infection and associated lesions in fully vaccinated women. Unresolved issues include the most critical groups to vaccinate and when the vaccine's cost may be low enough for widespread implementation in the developing world, where 80% of cervical cancer occurs.
Figures
References
-
- Pisani P., Parkin D.M., Munoz N., Ferlay J. Cancer and infection: estimates of the attributable fraction in 1990. Cancer Epidemiol. Biomarkers Prev. 1997;6:387–400. - PubMed
-
- Lowy D.R., Howley P.H. In Fields virology . D.M. Knipe and P.H. Howley, editors. Lippincott, Williams, & Wilkins.; Philadelphia, Pennsylvania, USA.: 2001. Papillomaviruses. pp. 2231–2264.
-
- Zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical application. Nat. Rev. Cancer. 2002;2:342–350. - PubMed
-
- Bosch F.X., Schiffman M., Solomon D. editors.Future directions in epidemiologic and preventive research on human papillomaviruses and cancer. J. Natl. Cancer Inst. Monogr. 2003;31:131. - PubMed
-
- Frisch M. On the etiology of anal squamous carcinoma. Dan. Med. Bull. 2002;49:194–209. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
