

Comparison of exercise, dobutamine-atropine and dipyridamole-atropine stress echocardiography in detecting coronary artery disease
- PMID: 16672046
- PMCID: PMC1475887
- DOI: 10.1186/1476-7120-4-22
Comparison of exercise, dobutamine-atropine and dipyridamole-atropine stress echocardiography in detecting coronary artery disease
Abstract
Background: Dipyridamole and dobutamine stress echocardiography testing are most widely utilized, but their sensitivity remained suboptimal in comparison to routine exercise stress echocardiography. The aim of our study is to compare, head-to-head, exercise, dobutamine and dipyridamole stress echocardiography tests, performed with state-of-the-art protocols in a large scale prospective group of patients.
Methods: Dipyridamole-atropine (Dipatro: 0.84 mg/kg over 10 min i.v. dipyridamole with addition of up to 1 mg of atropine), dobutamine-atropine (Dobatro: up to 40 mcg/kg/min i.v. dobutamine with addition of up to 1 mg of atropine) and exercise (Ex, Bruce) were performed in 166 pts. Of them, 117 pts without resting wall motion abnormalities were enrolled in study (91 male; mean age 54 +/- 10 years; previous non-transmural myocardial infarction in 32 pts, angina pectoris in 69 pts and atypical chest pain in 16 pts). Tests were performed in random sequence, in 3 different days, within 5 day period under identical therapy. All patients underwent coronary angiography.
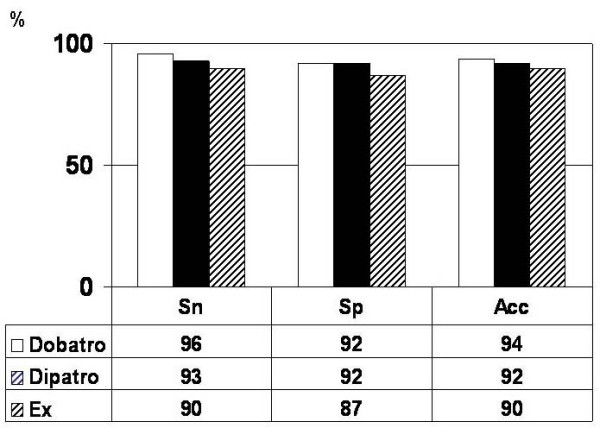
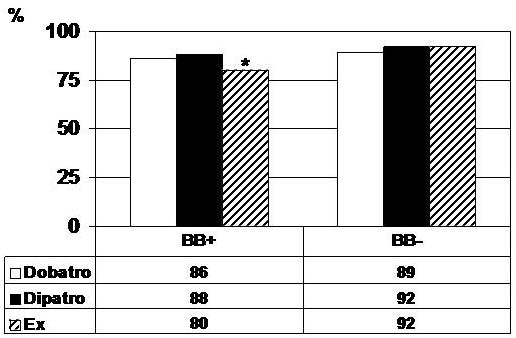
Results: Significant coronary artery disease (CAD; > or =50% diameter stenosis) was present in 69 pts (57 pts 1-vessel CAD, 12 multivessel CAD) and absent in 48 pts. Sensitivity (Sn) was 96%, 93% and 90%, whereas specificity (Sp) was 92%, 92% and 87% for Dobatro, Dipatro and Ex, respectively (p = ns). Concomitant beta blocker therapy did not influence peak rate-pressure product and Sn of Dobatro and Dipatro (p = ns).
Conclusion: When state-of-the-art protocols are used, dipyridamole and dobutamine stress echocardiography have comparable and high diagnostic accuracy, similar to maximal post-exercise treadmill stress echocardiography.
Figures
Similar articles
-
The diagnostic accuracy of pharmacological stress echocardiography for the assessment of coronary artery disease: a meta-analysis.Cardiovasc Ultrasound. 2008 Jun 19;6:30. doi: 10.1186/1476-7120-6-30. Cardiovasc Ultrasound. 2008. PMID: 18565214 Free PMC article. Review.
-
The atropine factor in pharmacologic stress echocardiography. Echo Persantine (EPIC) and Echo Dobutamine International Cooperative (EDIC) Study Groups.J Am Coll Cardiol. 1996 Apr;27(5):1164-70. doi: 10.1016/0735-1097(95)00586-2. J Am Coll Cardiol. 1996. PMID: 8609337 Clinical Trial.
-
Stress echocardiography in the detection of myocardial ischemia. Head-to-head comparison of exercise, dobutamine, and dipyridamole tests.Circulation. 1994 Sep;90(3):1168-76. doi: 10.1161/01.cir.90.3.1168. Circulation. 1994. PMID: 7916274 Clinical Trial.
-
Dipyridamole and dobutamine-atropine stress echocardiography in the diagnosis of coronary artery disease. Comparison with exercise stress test, analysis of agreement, and impact of antianginal treatment.Chest. 1996 Nov;110(5):1248-54. doi: 10.1378/chest.110.5.1248. Chest. 1996. PMID: 8915229 Clinical Trial.
-
Dipyridamole stress echocardiography: state of the art 1996. EPIC (Echo Persantin International Cooperative) Study Group.Eur Heart J. 1997 Jun;18 Suppl D:D16-23. doi: 10.1093/eurheartj/18.suppl_d.16. Eur Heart J. 1997. PMID: 9183606 Review.
Cited by
-
Dipyridamole stress echocardiography stratifies outcomes of asymptomatic patients with recent myocardial revascularization.Int J Cardiovasc Imaging. 2008 Jun;24(5):495-502. doi: 10.1007/s10554-007-9289-6. Epub 2007 Dec 22. Int J Cardiovasc Imaging. 2008. PMID: 18157613
-
Improved detection of ischemic heart disease by combining high-frequency electrocardiogram analysis with exercise stress echocardiography.Korean Circ J. 2013 Oct;43(10):674-80. doi: 10.4070/kcj.2013.43.10.674. Epub 2013 Oct 30. Korean Circ J. 2013. PMID: 24255651 Free PMC article.
-
Target heart rate to determine the normal value of coronary flow reserve during dobutamine stress echocardiography.Cardiovasc Ultrasound. 2011 Apr 4;9:10. doi: 10.1186/1476-7120-9-10. Cardiovasc Ultrasound. 2011. PMID: 21457582 Free PMC article.
-
The Ecto-5'-Nucleotidase/CD73 Inhibitor, α,β-Methylene Adenosine 5'-Diphosphate, Exacerbates Carrageenan-Induced Pleurisy in Rat.Front Pharmacol. 2019 Jul 11;10:775. doi: 10.3389/fphar.2019.00775. eCollection 2019. Front Pharmacol. 2019. PMID: 31354490 Free PMC article.
-
The diagnostic accuracy of pharmacological stress echocardiography for the assessment of coronary artery disease: a meta-analysis.Cardiovasc Ultrasound. 2008 Jun 19;6:30. doi: 10.1186/1476-7120-6-30. Cardiovasc Ultrasound. 2008. PMID: 18565214 Free PMC article. Review.
References
-
- Marwick T, Nemec J, Pashow F, Stewart WJ, Salcedo EE. Accuracy and limitation of routine exercise echocardiography in a routine clinical setting. J Am Coll Cardiol. 1992;19:74–81. - PubMed
-
- Ryan T, Vasey CG, Presti CF, O'Donnell JA, Feigenbaum H, Armstrong WF. Exercise echocardiography: Detection of coronary artery disease in patients with normal left ventricular wall motion at rest. J Am Coll Cardiol. 1988;11:993–999. - PubMed
-
- Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GE, Bierman FZ, Davis JL, Douglas PS, Faxon DP, Gillam LD, Kimball TR, Kussmaul WG, Pearlman AS, Philbrick JT, Rakowski H, Thys DM, Antman EM, Smith SC, Jr, Alpert JS, Gregoratos G, Anderson JL, Hiratzka LF, Faxon DP, Hunt SA, Fuster V, Jacobs AK, Gibbons RJ, Russell RO. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: Summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines on the Clinical Application of Echocardiography) J Am Coll Cardiol. 2003;42:954–970. doi: 10.1016/S0735-1097(03)01065-9. - DOI - PubMed
-
- Picano E, Distante A, Masini M, Morales MA, Lattanzi F, L'Abbate A. Dipyridamole echocardiography test in effort angina pectoris. J Am Coll Cardiol. 1985;56:452–456. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
